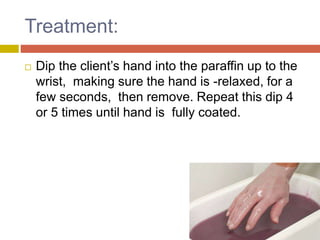
Paraffin wax therapy utilizes molten paraffin mixed with mineral oil for heat treatment, primarily to improve mobility in hands. It has a therapeutic temperature range of 42-50°C and is applied using methods like dip and wrap, providing benefits such as pain relief and increased blood circulation, although it has contraindications and requires proper precautions. Although effective for managing conditions like arthritis and muscle spasms, it is limited to distal extremities and cannot be used on open wounds.