Downloaded 142 times


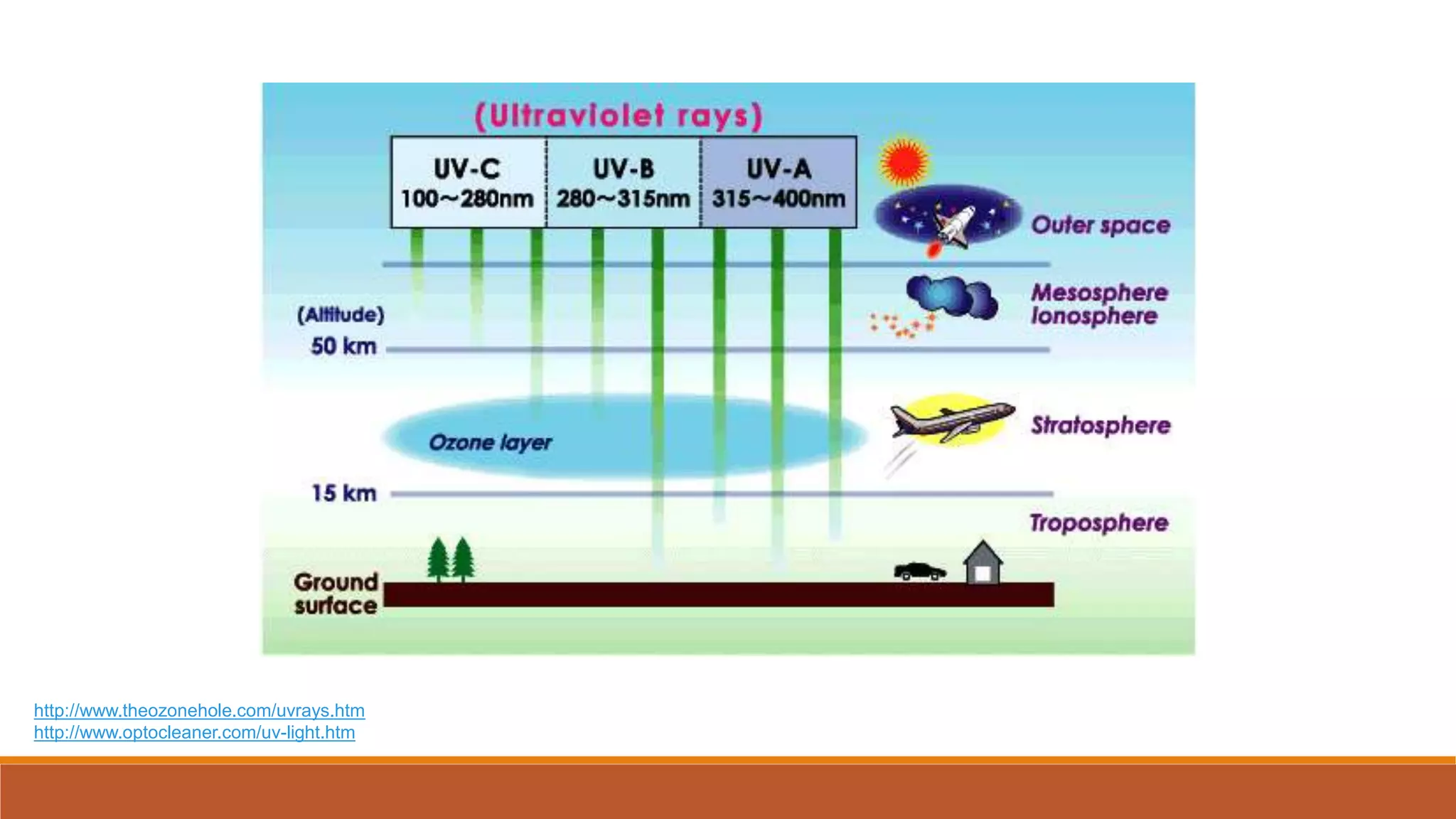
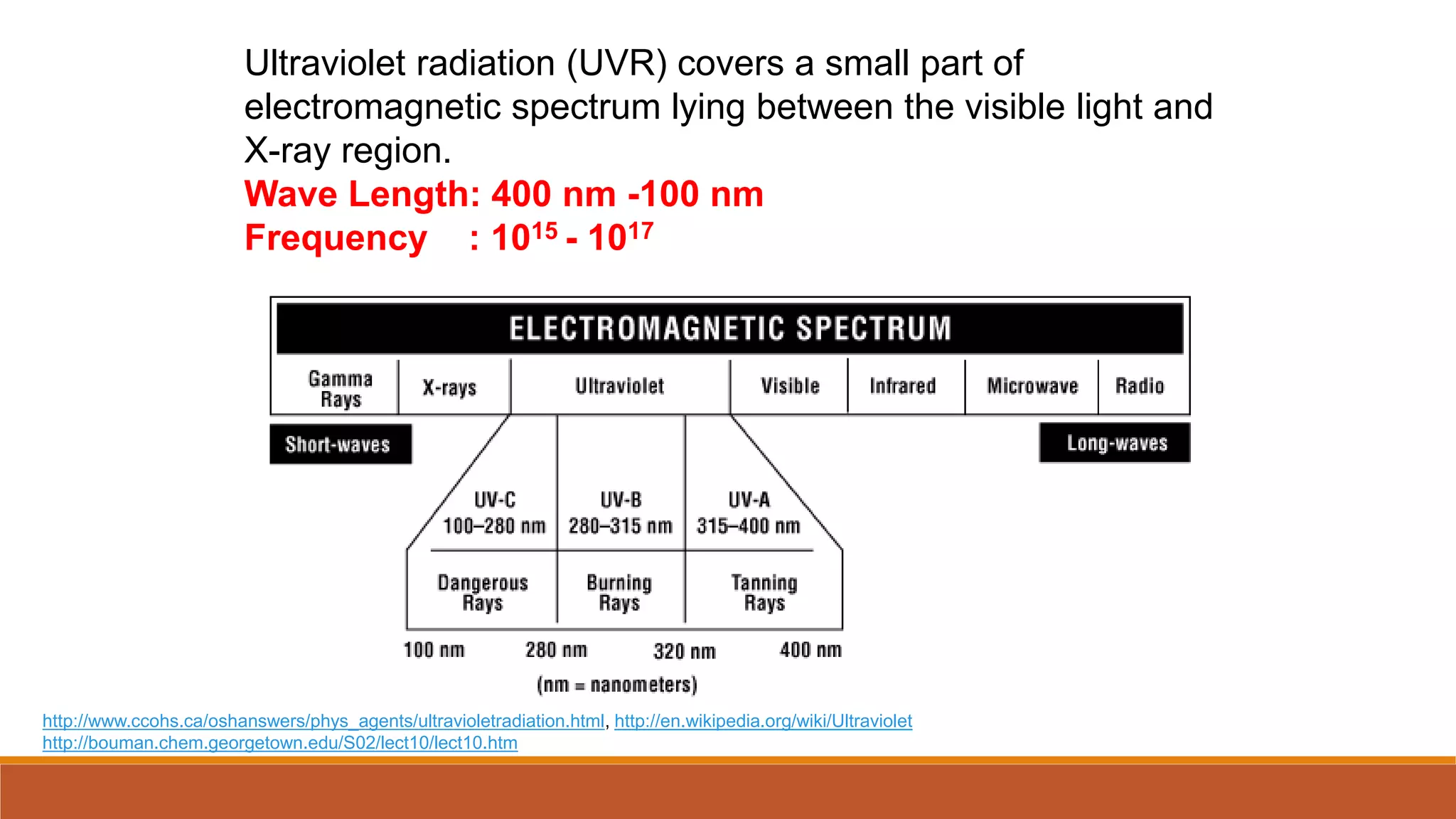
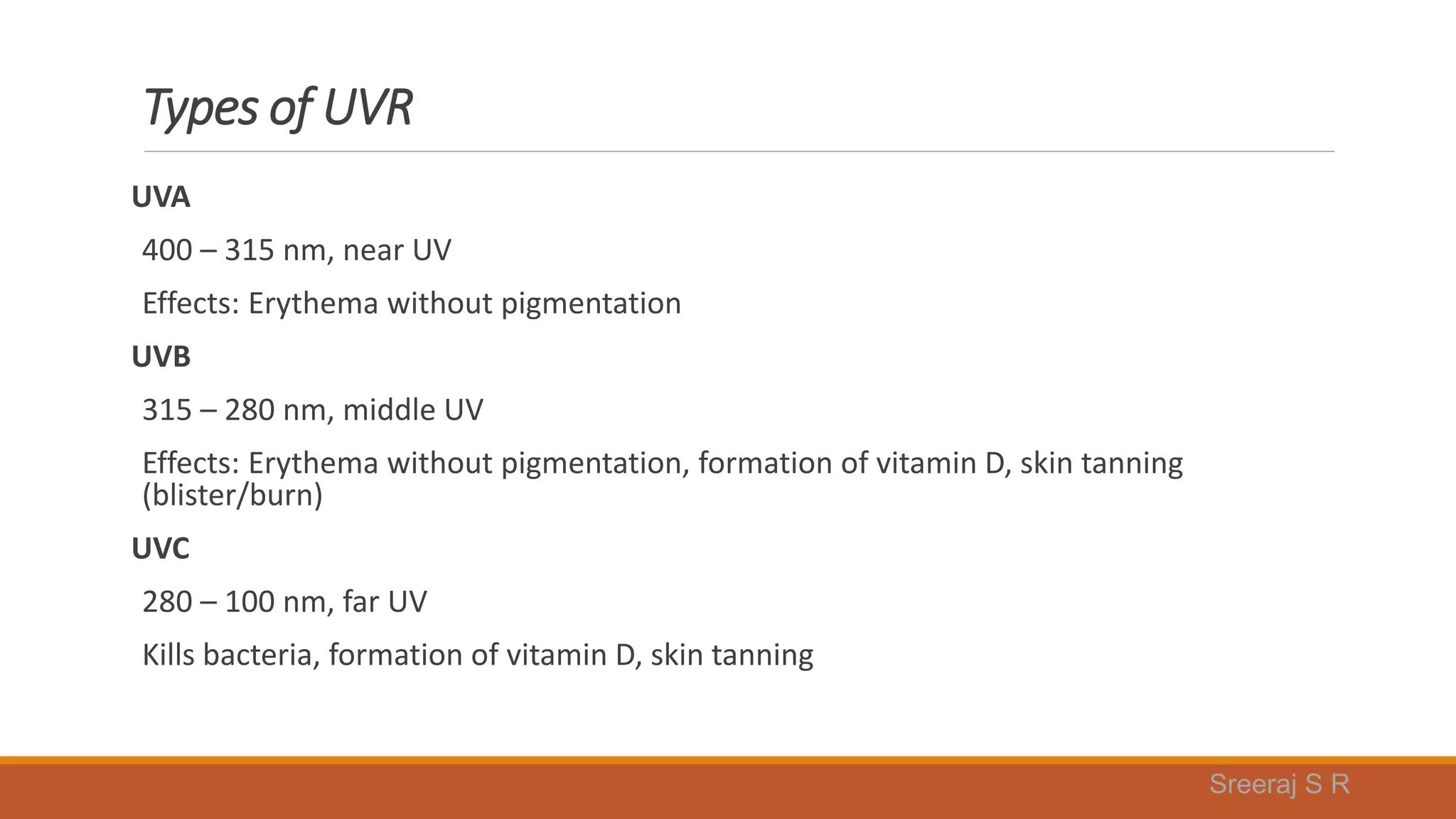


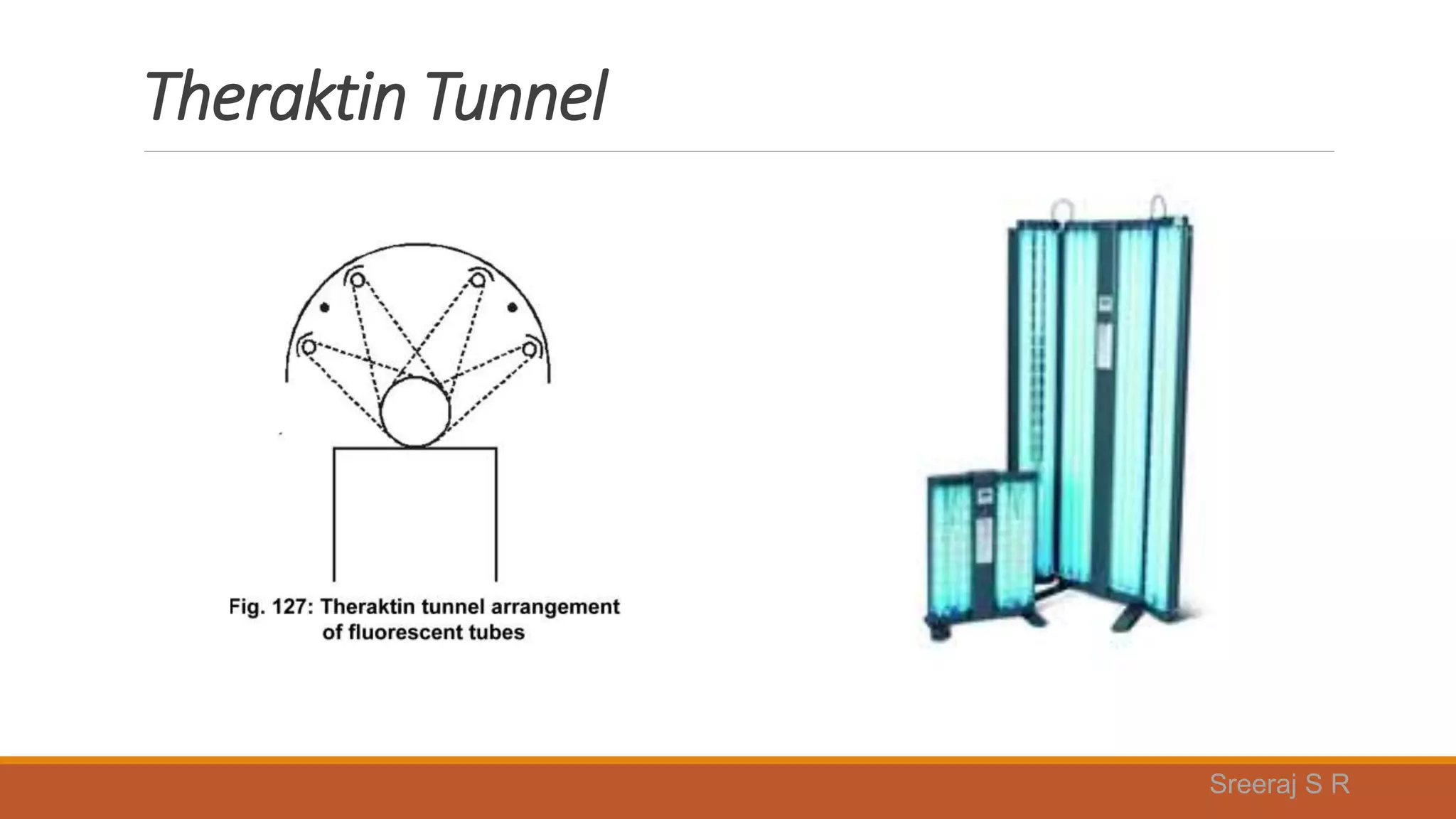


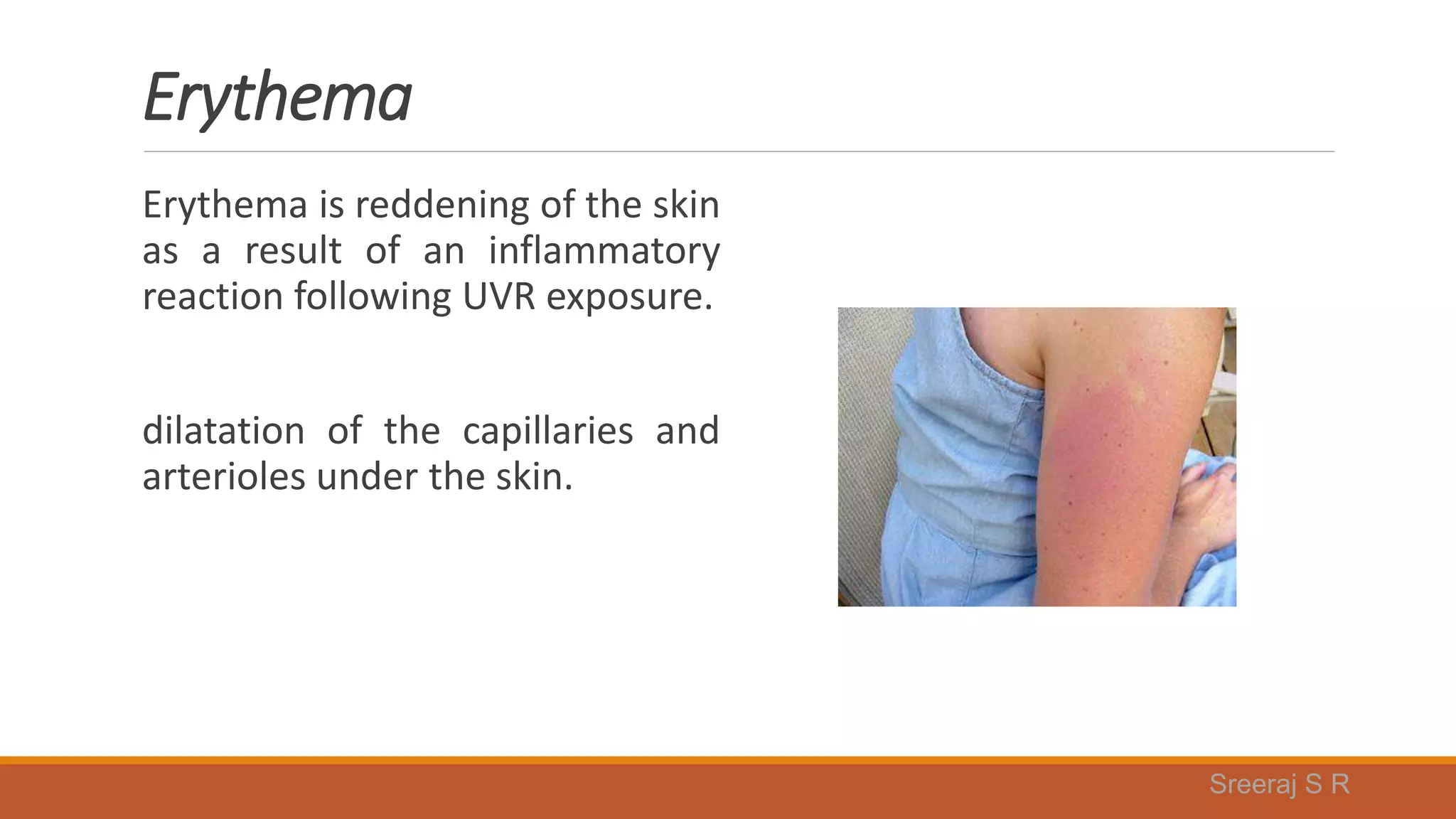
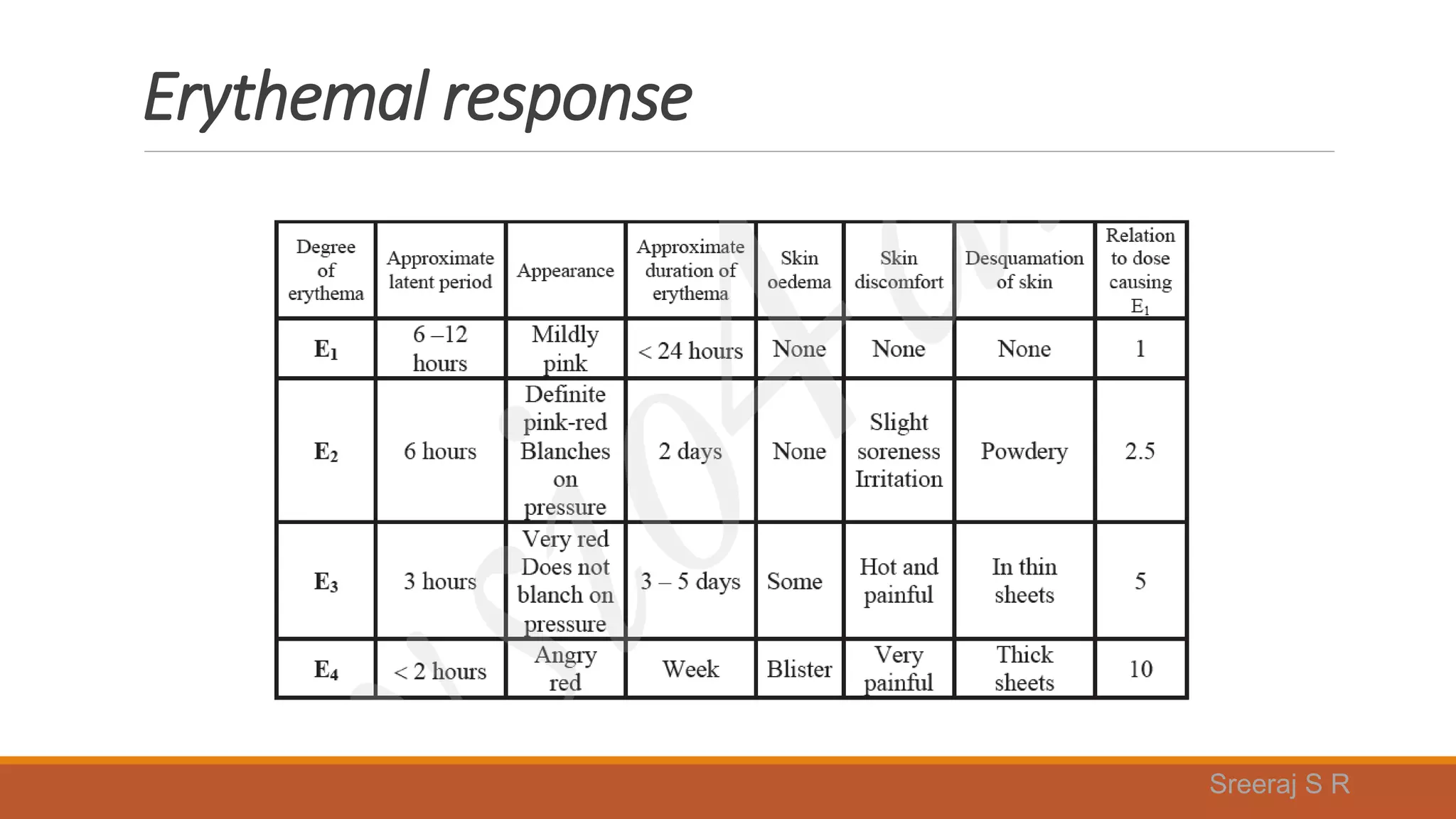






















Ultraviolet radiation covers a small part of the electromagnetic spectrum between visible light and X-rays. It is divided into UVA, UVB, and UVC based on wavelength. UV is produced by mercury vapor lamps and fluorescent lamps and can cause both immediate and long term effects on skin like erythema, pigmentation, vitamin D production, and skin cancer. The dosage of UV exposure depends on the lamp output, distance from the skin, exposure time, and individual skin sensitivity. UV therapy is used to treat conditions like psoriasis, acne, and eczema.























































































