Downloaded 338 times
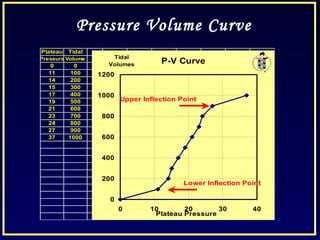
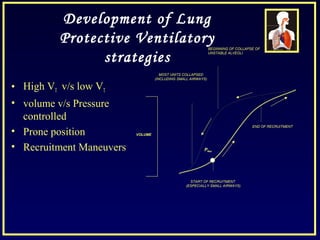
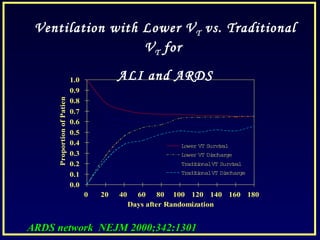
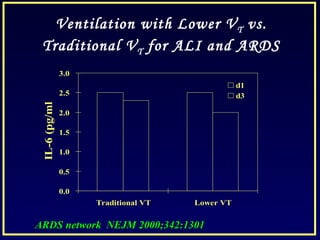
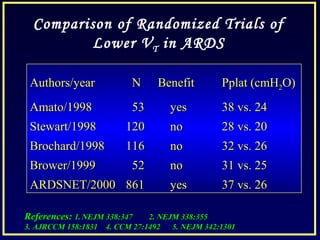
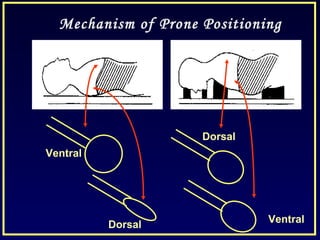
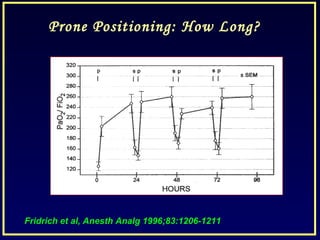
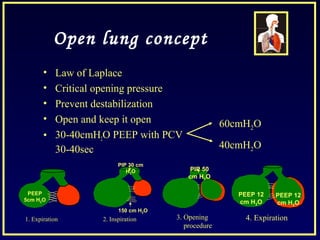

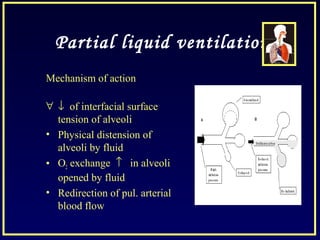


This document discusses various ventilatory strategies for treating ALI/ARDS, including: - Positive end-expiratory pressure (PEEP) which reduces atelectasis and improves oxygenation. - Controlled mechanical ventilation aims to decrease ventilatory inequalities and distribute flow better while limiting plateau pressure. - Low tidal volume ventilation as per the ARDSnet trial reduces mortality compared to conventional tidal volumes. - Recruitment maneuvers use high pressures to reopen collapsed alveoli but can cause barotrauma and hemodynamic instability if not done carefully. - Other strategies discussed include prone positioning, high frequency ventilation, airway pressure release ventilation and partial liquid ventilation. The goal is








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


