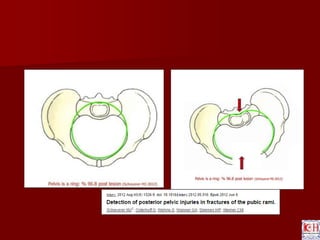
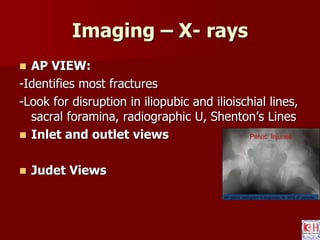
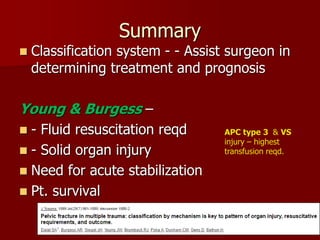
This document discusses pelvic ring fractures, including their epidemiology, anatomy, imaging, and classification. It notes that pelvic fractures are usually due to high-impact trauma and have a 10% overall mortality rate. The pelvis has both anterior and posterior ligamentous supports. Imaging includes x-rays, CT scans, and arteriograms. Several classification systems are described for categorizing fracture patterns based on injury mechanism, including the Young-Burgess system which divides fractures into lateral compression, anteroposterior compression, and vertical shear patterns. The classification helps determine treatment and prognosis, with anteroposterior compression type 3 and vertical shear fractures having the highest transfusion requirements.










































![Management of pelvic ring fractures [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofunstablepelvicfracturesautosaved-180101211035-thumbnail.jpg?width=640&height=640&fit=bounds)


























































































