Downloaded 36 times


















![
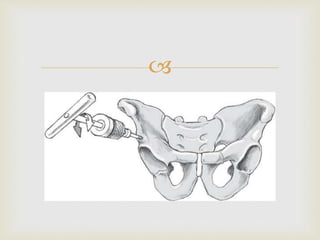
The orientation of the ala of the iliac bone
is determined by palpation with
an instrument [30], a Kirschner wire [28] or
the finger. Only the cortical bone
is perforated by the drill bit, and the
Schanz screw is then introduced into
the drill hole and further advanced
between the two laminae of the iliac
bone without predrilling.](https://image.slidesharecdn.com/pelvicexfix-160403173523/85/Pelvic-ex-fix-27-320.jpg)
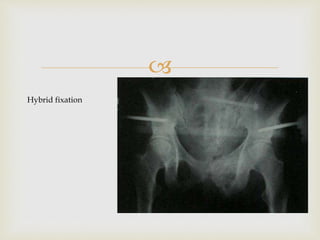





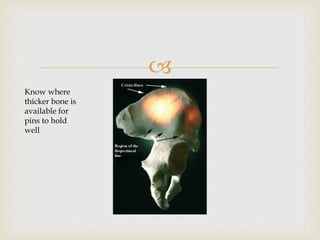
This document discusses the use of external fixation for pelvic injuries. It notes that external fixation is commonly used for emergency stabilization of pelvic ring injuries. While it provides adequate stability for some types of injuries, its stability is poor for vertically unstable type C injuries. External fixation is best as a temporary measure in the emergency department or as part of a hybrid fixation approach combined with internal fixation. Placement of screws in the supra-acetabular region is preferred to the iliac crest for better holding power and soft tissue coverage.























































































