The document discusses pelvic fractures, their classification, causes, symptoms, diagnostic process, and treatment approaches. Some key points:
- Pelvic fractures account for 3% of skeletal fractures and are usually caused by minor trauma, with higher mortality from severe trauma due to hemorrhage.
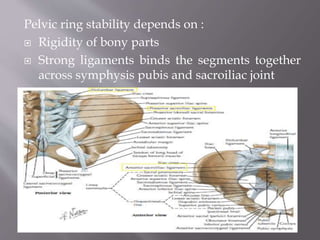
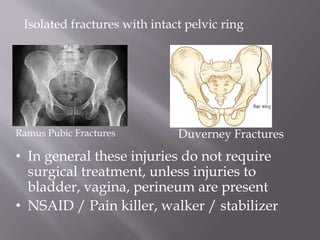
- Fractures are classified based on location (e.g. sacrum), stability (intact ring, broken ring), and mechanism of injury (compression, shear).
- Diagnosis involves imaging like x-rays and CT scan to identify fracture patterns and instability.
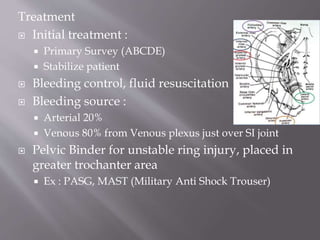
- Treatment depends on factors like displacement, stability, and injury severity. It may involve stabilization, external fixation, angiography, or surgery like
























































































![Management of pelvic ring fractures [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofunstablepelvicfracturesautosaved-180101211035-thumbnail.jpg?width=640&height=640&fit=bounds)


































