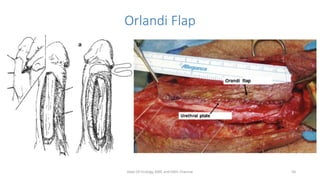
This document discusses stricture urethra and its management. It provides details on the epidemiology, etiology, clinical evaluation and surgical options for urethral strictures. Key points include that bulbar strictures are the most common, iatrogenic causes have increased in prevalence, clinical evaluation involves uroflowmetry, retrograde urethrogram and cystoscopy, and surgical options range from dilation and direct visual internal urethrotomy for short strictures to various types of urethroplasty using grafts or flaps for longer or complex strictures.