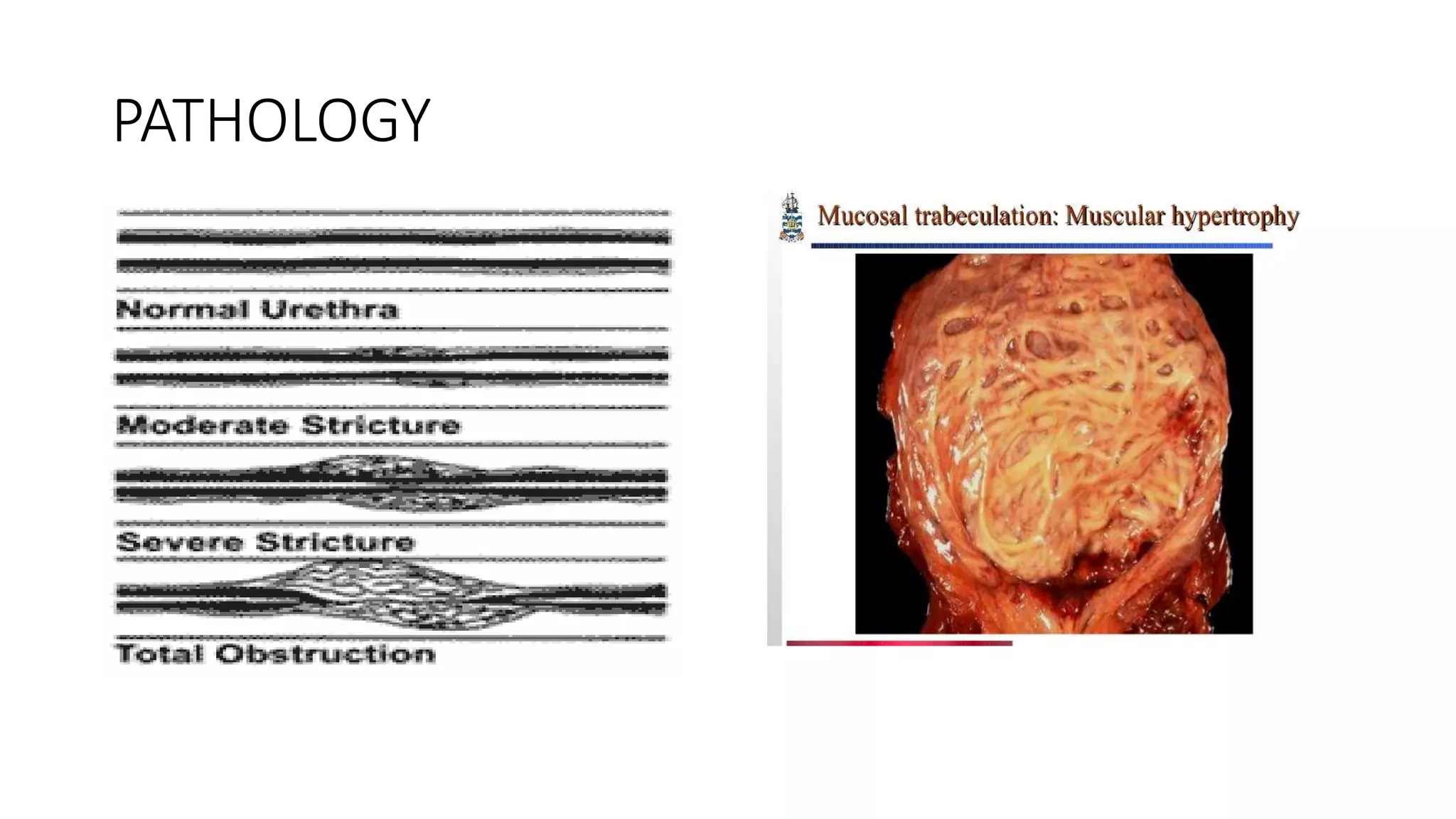
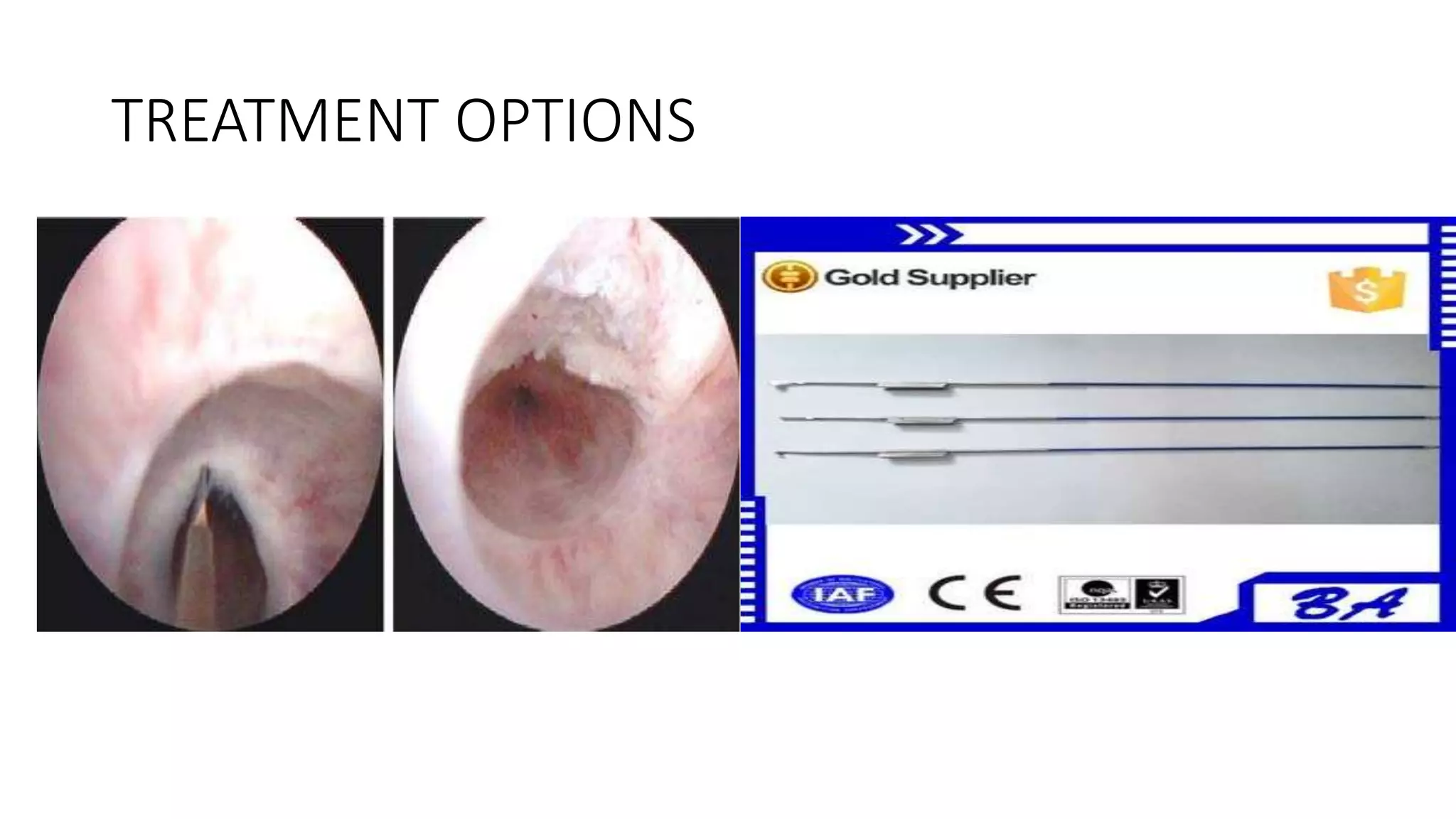
Urethral stricture is an abnormal narrowing of the urethra caused by fibrosis due to injury or inflammation. It is most common in males and usually occurs around age 50. Symptoms include poor urine stream and retention. Diagnosis involves tests like cystoscopy and retrograde urethrogram. Treatment depends on location and severity but may include dilation, internal urethrotomy, or open urethroplasty surgery to repair or bypass the stricture. Effective drainage of the bladder is important to manage this condition.