Male Urethra –Overview
• Fibromuscular tube extending from bladder
neck to external urethral meatus
• Length ≈ 18–20 cm
• Dual function:
– Conduction of urine
– Conduction of semen during ejaculation
3.
Functions of MaleUrethra
• Urinary excretion from bladder
• Passage of semen from ejaculatory ducts
• Role in continence and ejaculation
External Urethral Meatus
• Vertical, slit-like opening
• Located at tip of glans penis
• Narrowest part of urethra
4.
Parts of theMale Urethra
• Prostatic urethra
• Membranous urethra
• Spongy (penile) urethra
• The glandular part of the urethra is called the
fossa navicularis.
Penile (Spongy) Urethra
•Extends from meatus to penoscrotal junction
• Surrounded by corpus spongiosum
• Conveys urine and semen
7.
Bulbar Urethra
• Extendsfrom penoscrotal junction to
bulbomembranous junction
• Lies within bulb of penis
• Surrounded by corpus spongiosum
• Common site for urethral injuries and
strictures
8.
Membranous Urethra
• Extendsfrom bulbomembranous junction to
verumontanum
• Shortest and least distensible part
• Surrounded by external urethral sphincter
– Smooth muscle sphincter
– Striated Rhabdosphincter
• Pudendal nerve, originating from spinal
segments S2–4.
9.
External Urethral Sphincter
•Voluntary sphincter
• Innervated by pudendal nerve (S2–S4)
• Important for urinary continence
10.
Prostatic Urethra
• Extendsfrom bladder neck to
verumontanum
• Surrounded by prostate gland
• Receives ejaculatory ducts at verumontanum
11.
Bladder Neck
• Actsas internal (genital) sphincter
• Closes during ejaculation → prevents
retrograde ejaculation
• Contributes to continence
• Functions independently of external sphincter
12.
STRICTURE URETHRA
• ClassificationI: Aetiologically.
1. Congenital.
2. Inflammatory:
• a. Post-gonococcal is most common (70%).
– Gonococcal stricture occurs one year after
infection.
– Retention develops only 10–15 years later.
– Common in the bulb of urethra especially in the
roof.
• b. Tuberculous.
• c. Other infection (urethritis).
13.
3. Traumatic: Bulbous,membranous.
4. Post-instrumentation: Catheter, dilator,
cystoscope.
5. Postoperative: Prostate surgery (4%),
urethrostomy
Classification II:
1. Proximal: Common in bulbous urethra (70%).
2. Distal: Congenital (in the external meatus).
Often traumatic in children
14.
Classification III:
1. Permeable:Permits urine to pass.
2. Impermeable.
Classification IV:
1. Passable: Allows catheter to pass.
2. Impassable.
Classification V: It can be single or multiple.
Classification VI: According to the part involved.
In the roof (most common) or in the floor
15.
Clinical features
• Poorurinary stream
• Forking and spraying of the stream
• Incomplete emptying
• Frequency, dysuria
• Retention and often with overflow
• Pain, burning micturition, suprapubic tenderness
• Thickening and button-like feeling in bulbar
urethra (Bulbous urethra is felt clinically by lifting the
scrotum in midline in the perineum)
16.
Investigations
• Urine microscopyand culture
• Blood urea and serum creatinine.
• IVU (Intravenous Urography)to see
hydronephrosis and function of kidney.
• Ultrasound abdomen.
• X-ray of pelvis to see old fracture with history
of trauma.
• Urodynamic studies.
• Urethroscopy.
17.
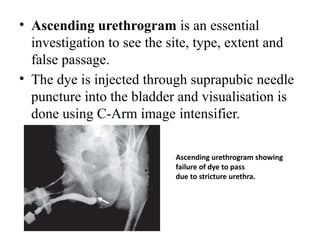
• Ascending urethrogramis an essential
investigation to see the site, type, extent and
false passage.
• The dye is injected through suprapubic needle
puncture into the bladder and visualisation is
done using C-Arm image intensifier.
Ascending urethrogram showing
failure of dye to pass
due to stricture urethra.
Treatment
1. Intermittent dilatation:
•Gradual dilatation, initially with thin dilators,
later with
thicker dilators of increasing size. Dilatation
should be done in OT under aseptic precaution.
• Should avoid forcible dilatation or over
dilatation.
• Dilatation is done “Once a week for one
month, once a month for one year, and later
once a year (on his birthday)”.
20.
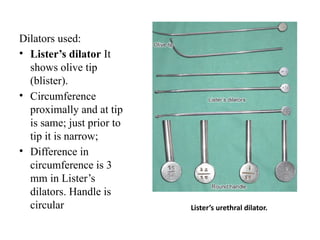
Dilators used:
• Lister’sdilator It
shows olive tip
(blister).
• Circumference
proximally and at tip
is same; just prior to
tip it is narrow;
• Difference in
circumference is 3
mm in Lister’s
dilators. Handle is
circular Lister’s urethral dilator.
21.
• b. Clutton’sdilator. c. Filiform bougies.
Clutton’s dilator.
It is violin shaped; does not have olive tip;
gradually narrows towards tip;
Difference in circumference proximal to
distal is 4 mm; handle is violin like. Filiform bougies are used to dilate
narrow stricture urethra.
One of the bougies will be passed
into the urethra.
2. Visual internalcystoscopic urethrotomy or
stricturotomy:
• Here using cystoscope, stricture is visualised
and is cut at 12 o’clock position, until it bleeds
(fibrous tissue is cut completely).
• After that Foley’s catheter is passed and kept
in position for 48 hours.
24.
3. External urethrotomyby open method.
• Presently not commonly done as cystoscopic
urethrotomy is more popular.
• It is presently done as an initial stage surgery
for urethroplasty (Wheelhouse’s operation).
4. Urethroplasty: Stricture is excised and
urethra is reconstructed using prepuceal skin or
scrotal skin (Johanson’s urethroplasty)
25.
Problems in urethroplasty
•Staged procedure and so prolonged
hospitalisation
• Infection
• Necrosis of skin flap
• Leak and fistula formation
• Restenosis
26.
Complications of strictureurethra
• Retention of urine
™
• Urethral fistula
• Infection—urethritis, cystitis, pyelonephritis
• Urethral diverticula
• Periurethral abscess
• Bilateral hydronephrosis
• Stone formation
• Renal failure
• Due to straining—hernia, haemorrhoids, rectal
prolapse
27.
Anatomy of FemaleUrethra
• The female urethra is around 4cm long,
extending from the bladder neck to the meatus.
• The entire length of female urethra is sphincter
active.
• There is extra support from the surrounding
pelvic floor musculature.
Caruncle
• This isseen in elderly women.
• It presents as a soft, raspberrylike
mass about the size of a pea.
• It is actually the prolapsed
urethral mucosa at the 6 o’clock
position
• If required it is treated by
excision and diathermy
coagulation of the base of the
stalk.
30.
• Stricture
• Urethralstricture is uncommon in women.
• The aetiology includes urethritis, trauma
associated with a prolonged or difficult labour
or instrumentation.
• The strictureis initially managed by urethral
dilatation.
• Urethroplasty with buccal mucosa
augmentation is advocated for recurrent
strictures.
31.
• Diverticulum
• Afemale urethral diverticulum may be
congenital or caused by rupture of a distended
and infected paraurethral gland
• or by injury of the urethra during childbirth.
• Urine within the diverticulum becomes
infected, causing local pain and repeated
bouts of cystitis.
• Purulent urine is discharged if the urethra is
compressed with a finger placed in the vagina.
32.
• Diagnosis isby MRI or by transvaginal
ultrasound.
• Excision of the diverticulum through the
anterior vaginal wall is effective,
• but care must be taken not to damage the
urethral sphincter
(a) Magnetic resonance imaging showing
a diverticulum arising from the
posterior wall of the urethra.
(b) It appears bright owing to
accumulated urine and infected
material (arrow).
33.
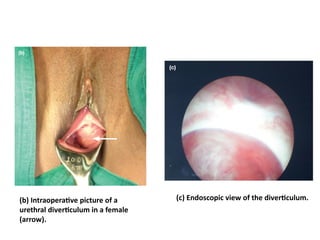
(b) Intraoperative pictureof a
urethral diverticulum in a female
(arrow).
(c) Endoscopic view of the diverticulum.
34.
URETHRAL INJURY
Classification
I. Dependingon site of rupture:
1. Rupture of the membranous urethra.
2. Rupture of the bulbous urethra.
II. Depending on circumference of the urethral wall
involved:
1. Complete.
2. Incomplete.
III. Depending on the thickness of the urethra involved:
1. Total.
2. Partial.
35.
RUPTURE OF MEMBRANOUSURETHRA
and/or Prostatic urethra (Posterior Urethra)
Causes
• It is usually associated with Pelvic fracture,
commonly due to road traffic accidents
• Injury can also occur during instrumentation
™
• Calculus passage and catheterisation
• In prolonged labour, due to long-standing
pressure on the urethra by foetal head
36.
• Prostate isattached to pubis by puboprostatic
ligament and disruption of puboprostatic
ligament with complete rupture of urethra can
lead to floating prostate—Vermooten’s sign.
• Injury can lead to incomplete rupture of
urethra or may be associated with
extraperitoneal rupture of bladder.
37.
Based on ascendingurethrogram, posterior
urethral injury is classified as (Mccallum-
colapinto classification).
• Type I: Elongation of posterior urethra, but intact
• Type II: Prostate “plucked off’’ membranous
urethra with extravasation of urine above
sphincter only—Floating prostate—Vermooten’s
sign
• Type III: Total disruption of urethra with
extravasation of urine both above and below the
sphincter
38.
Clinical Features
• Bloodin external meatus. Failure or difficulty in
passing urine.
• Extravasation of urine to scrotum, perineum and
abdominal wall.
• Shock with pallor, tachycardia, hypotension.
• Features of associated injuries like head injury, thorax
and abdominal organs which take priority in initial
phases of management.
• On perrectal (PR) examination, prostate may be felt
high or may not be palpable at all. Signifies floating
prostate.
39.
• Investigations
• X-raypelvis to see for fracture.
• Ultrasound abdomen to see pelvis and other
injuries.
• Urethrogram is done to see the site and type of
tear (often reserved to do at later stage).
40.
A retrograde urethrogramand
voiding cystourethrogram
in a patient with a pelvic fracture
urethral injury showing the gap. The
bladder along with the prostate is
displaced upwards and there is a
gap between the bulbar urethra and
membranous urethra.
41.
Treatment
• The shockand associated injuries are treated.
In floating prostate:
• As rupture is complete, bladder is opened from
above.
• A metal bougie is passed from above through the
bladder and one more metal bougie is passed from
below through urethra and both are manipulated so as
to meet each other.
• Lower bougie is negotiated along the upper one and
so into the bladder. Red rubber catheter is tied to the
tip of the lower (urethral) bougie which has already
entered into the bladder.
42.
• When lowerbougie is pulled out per
urethrally, catheter tied to it will pass through
urethra from above, to which Foley’s catheter
is tied and pulled up, so as to keep it in
position.
• Bladder is closed with a SPC using Malecot’s
catheter—Railroad technique.
43.
In incomplete rupture:Two approaches:
1. First approach proposed by Mitchell:
• Do not pass catheter from below as it may
further damage the urethra and also may damage
sphincter mechanism and so may cause
incontinence later.
• Here SPC is done using Malecot’s catheter.
• After three to six weeks, an urethrogram is done.
Using endoscope or along with open method
Foley’s catheter is passed, often after dilatation
44.
2.Second approach advocatedby Blandy:
• Single attempt to pass a small soft catheter per
urethrally gently may lead into the bladder,
which will be kept in situ, to maintain the
continuity.
• If this fails SPC is done.
• On second day, in operation theatre (OT),
bladder is opened from above and flexible
cystoscope is passed from below and using
this, catheter is passed from below.
• Bladder is closed with a SPC.
45.
• If patientwith incomplete rupture presents
later, then it is managed once a stricture forms,
accordingly as stricture urethra, after 3
months.
• Until then patient may require SPC.
• Other measures: Antibiotics, blood, fluid
replacement, treatment of other injuries.
46.
• Complications
• Urinaryincontinence
• Impotence
• Stricture urethra
• Infection
™
Penetrating injury in the perineum causing
rectal and
urethral injury which is communicating.
Note the catheter passed
per urethra has gone into the rectum and
come out through the anal
canal. It needed colostomy and suprapubic
cystostomy diversions
47.
RUPTURE OF BULBOUSURETHRA
(Anterior Urethra)
• Usually, due to a fall astride a projecting
object, like in sailing ships, cycling, over loose
manhole cover, gymnasium.
• Rupture may be complete or incomplete.
• Total or partial.
48.
• Clinical features:Triad
• ™Blood in external meatus (Urethral
haemorrhage)
• Perineal haematoma
• Retention of urine
49.
Treatment
• Patient shouldbe told not to try to pass urine,
if passed, then extravasation of urine occurs.
• In operation theatre, one attempt of urethral
catheterisation is tried gently. If able to pass a
catheter, then it is left in place
• Often perineal haematoma which occurs, has
to be drained.
50.
• Antibiotics shouldbe given to prevent sepsis.
• If catheter fails to pass, then under general
anaesthesia, in lithotomy position, SPC is done.
• Bulbous urethra is exposed through perineal
midline incision and tear is sutured with an
indwelling Foley’s catheter.
• Drain is then placed into the perineum.
• If suturing is not possible (sometimes), then
perineal urethrostomy is done and at later stages
continuity is maintained (usually after 3 months).