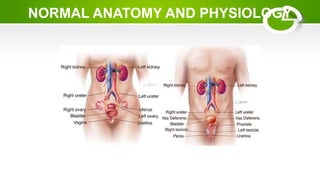
The document discusses urethral stricture, a condition characterized by the narrowing of the urethral lumen, commonly due to scarring from various causes such as infections, trauma, and surgeries. It outlines the anatomy and physiology of both male and female urethras, the epidemiology of the condition, symptoms, clinical diagnosis methods, and management strategies. Key treatments include catheterization, dilation, and urethroplasty, while early detection and addressing underlying causes are emphasized for prevention.