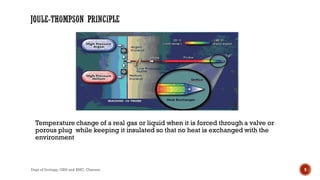
This document provides information about cryotherapy as a treatment for prostate cancer from the Department of Urology at Govt Royapettah Hospital and Kilpauk Medical College in Chennai, India. It discusses the mechanisms of cryotherapy, how it is performed, outcomes, and complications. Cryotherapy uses freezing to induce coagulative necrosis in prostate cancer by damaging cells through mechanisms like protein denaturation and rupture of cell membranes from expanding ice crystals. It can be used to treat localized prostate cancer as an alternative to radical treatments like surgery or radiation. Common side effects include erectile dysfunction, urinary incontinence, and urethral sloughing.

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





