Download as PDF, PPTX
















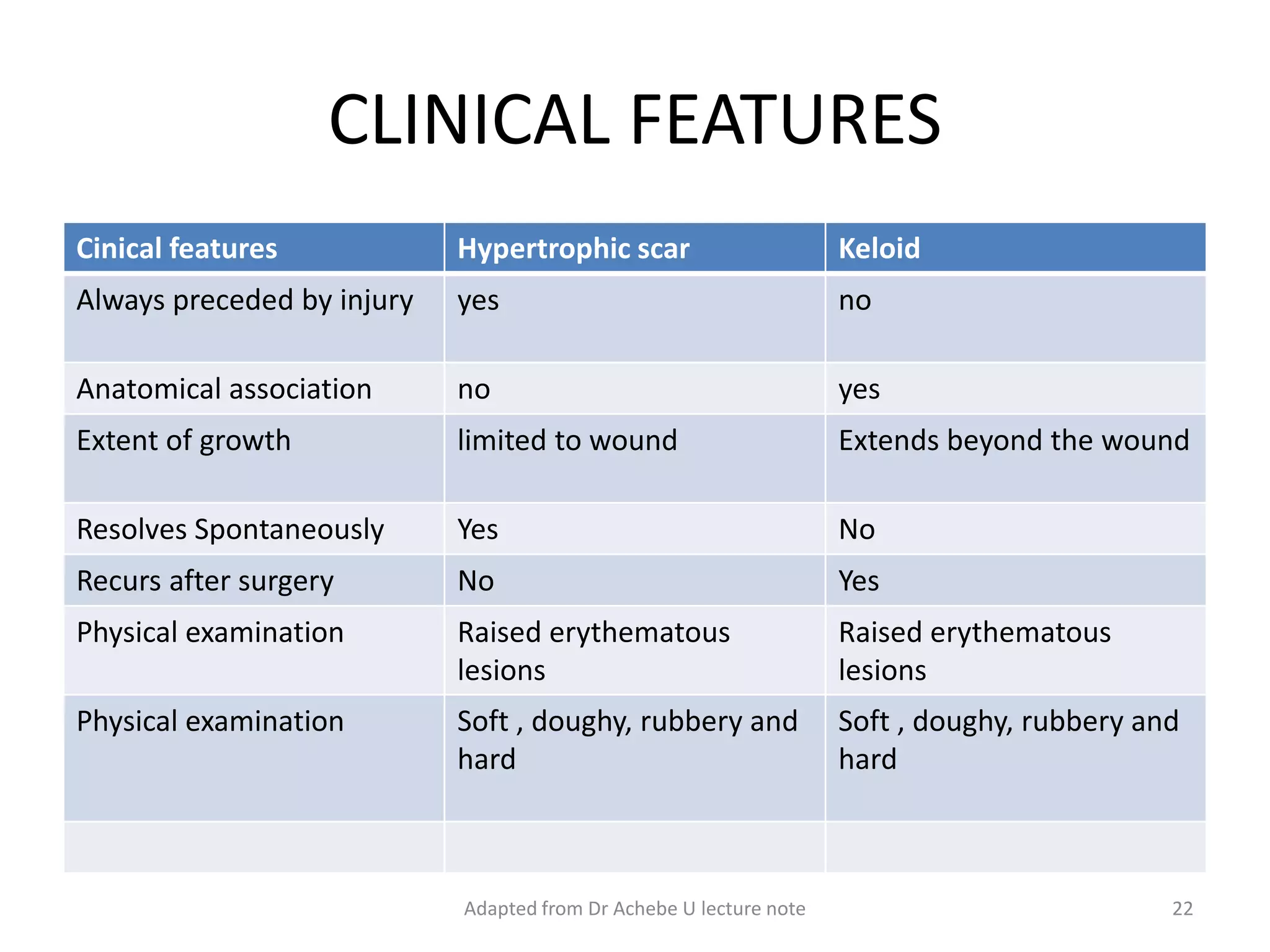
























This document discusses keloids and hypertrophic scars. It begins by defining each condition and providing an introduction. It then covers risk factors, pathogenesis, clinical features, diagnosis, management, prevention, complications, prognosis, and local experience. Keloids extend beyond the original wound site, while hypertrophic scars do not but are still raised and thickened. Risk factors include skin injury, genetics, and skin pigmentation. Management involves a variety of options depending on the case, often combining excision, steroid injection, and pressure therapy. Recurrence is a challenge, and further research is still needed for effective keloid treatment.















































































