Downloaded 1,589 times

![AMNIOTIC FLUID Amnionitic fluid evaluation allows assessment of the fetal intrauterine environment Potentially invaluable information Requires close follow-up and evaluation secondopinion2.com [email_address]](https://image.slidesharecdn.com/amnioticfluid-120212085244-phpapp01/75/Amniotic-fluid-43-2048.jpg)

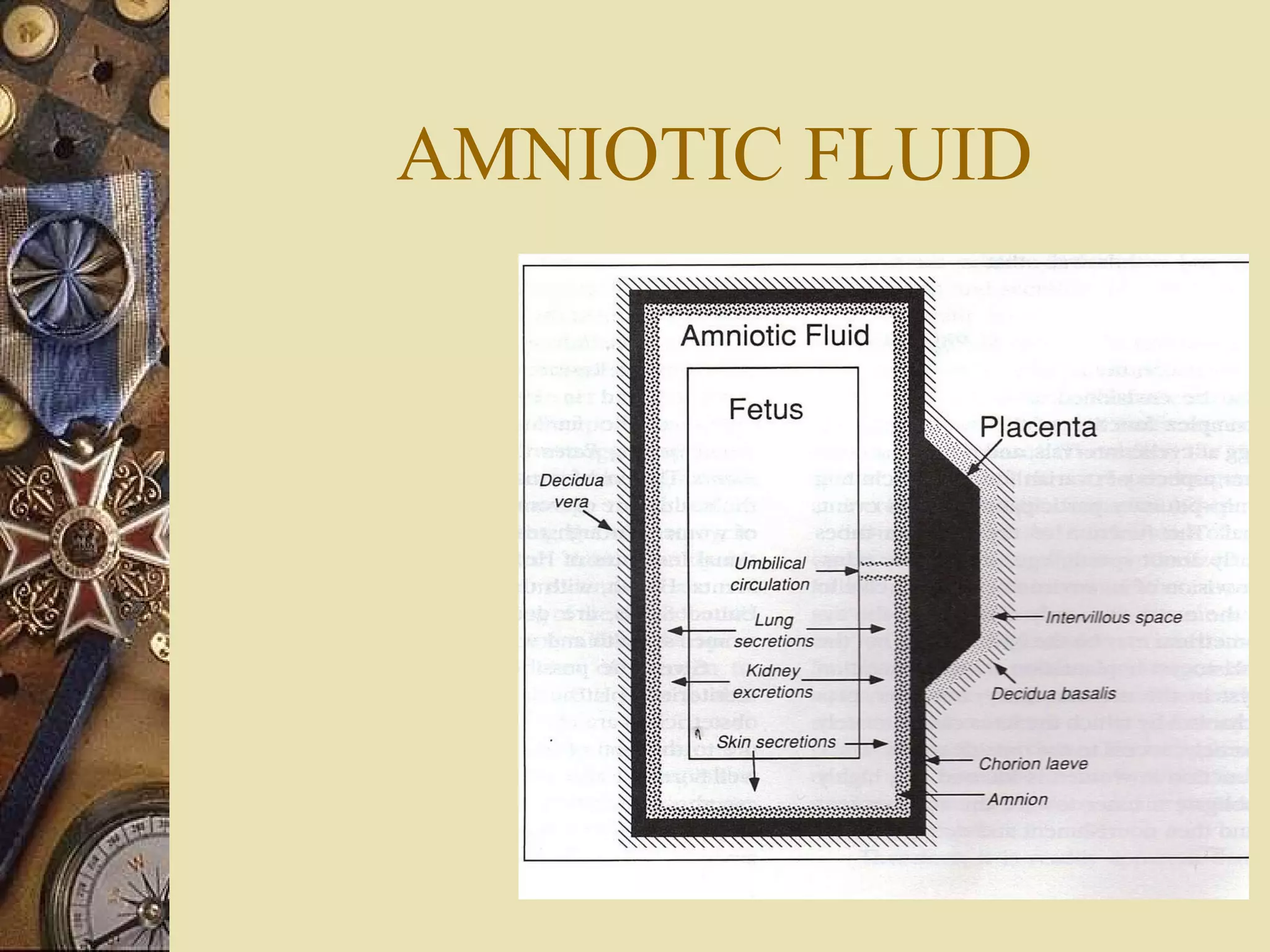
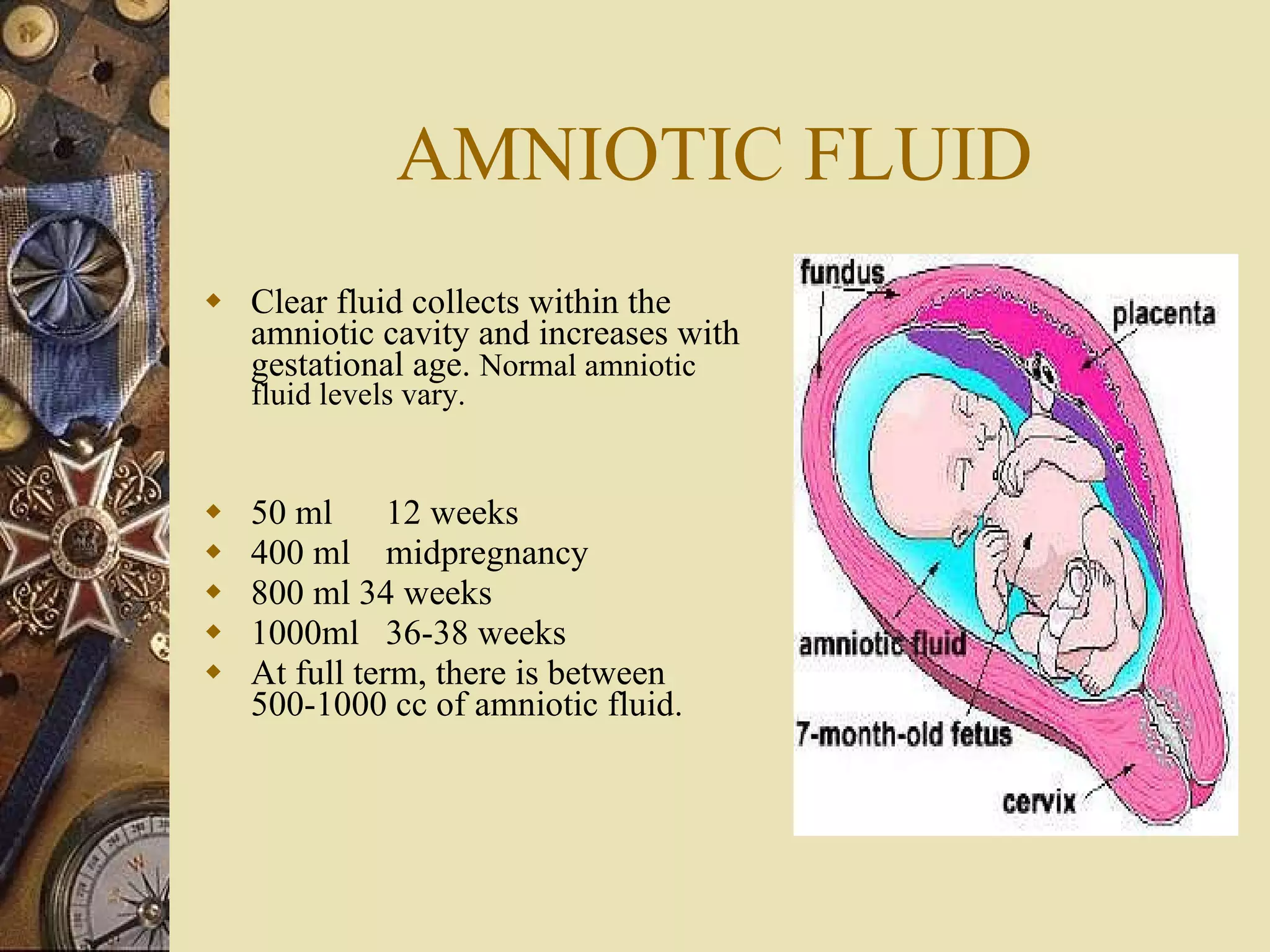
The amniotic fluid cushions the fetus, protects it from infection and trauma, and allows freedom of movement. It maintains a stable temperature and permits lung development. Amniotic fluid volume is normally 500-1000cc at term. It is produced by the amniotic membranes and passes across the fetal skin and through fetal urination, swallowing, and respiratory secretions. Abnormal volumes can indicate fetal problems and complications in pregnancy.