Download as PDF, PPTX
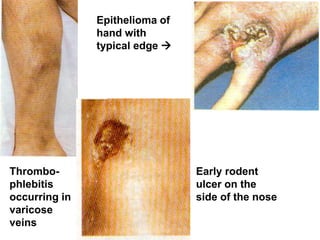
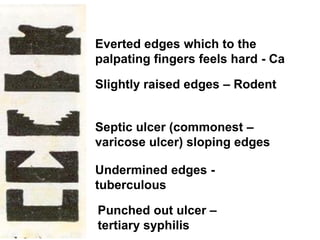
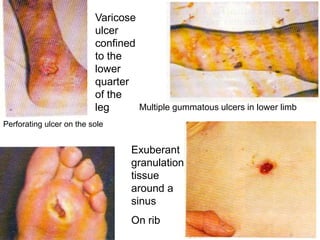
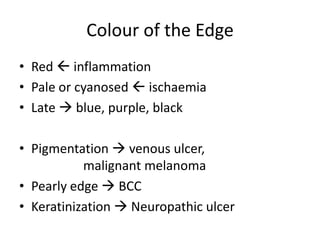
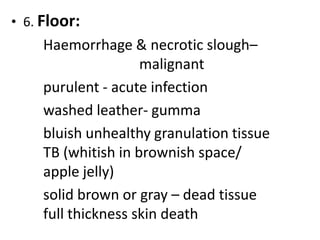
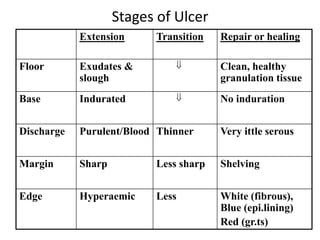


1. Ulcers are breaks in the skin or mucosa that can be caused by infections, trauma, vascular issues, neuropathy, cancer, or other factors. Diagnosis involves examining the ulcer's characteristics, patient history, and potentially investigations or a biopsy. 2. Treatment depends on the underlying cause but the stages of an ulcer include the extension, transition, and repair phases involving changes to the floor, edges, discharge, and surrounding tissue. 3. The next lecture will cover sinuses and fistulae and include an assessment test on wound healing.























































































