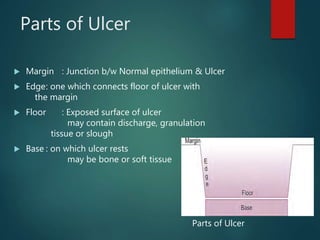
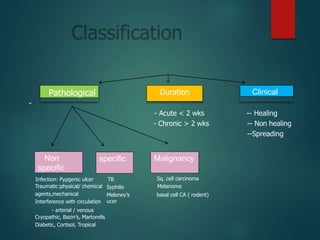
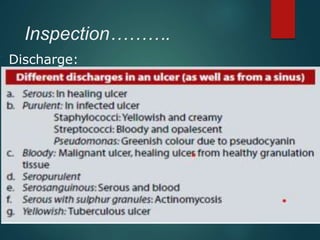
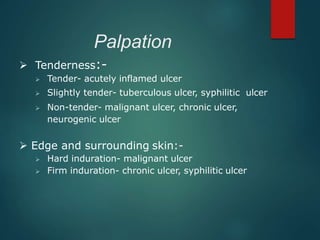
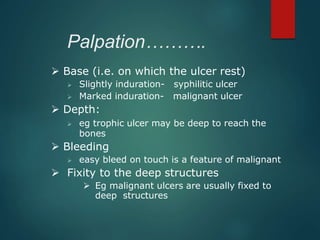
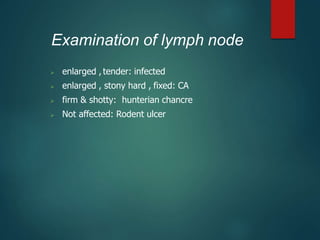
Ulcer is a break in the skin or mucous membrane. There are several types of ulcers including acute, chronic, spreading, and non-healing ulcers. Ulcers can be caused by infection, trauma, poor circulation, or underlying conditions like diabetes. The key parts of an ulcer include the margin, edge, floor, and base. Evaluation of an ulcer involves examining these parts and considering characteristics like appearance, drainage, surrounding skin, and tenderness. Investigation and management depends on the identified cause, with goals of cleaning the ulcer, promoting healing, treating underlying issues, and closing the wound.




































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











