Downloaded 880 times







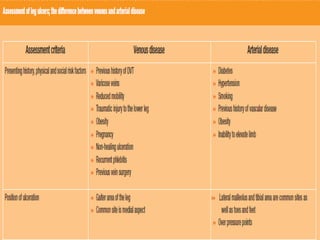
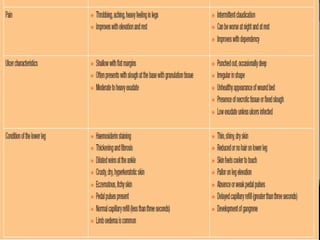
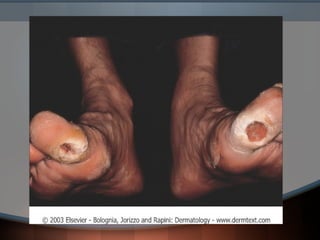
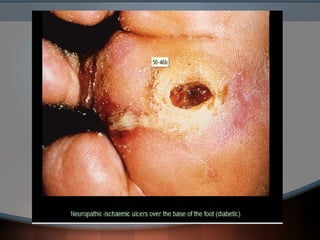
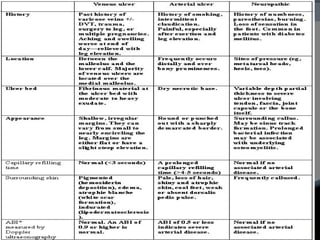




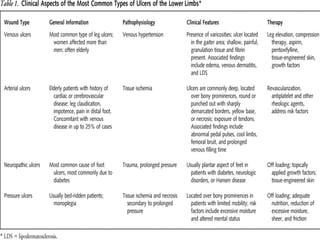


This document discusses different types of leg ulcers including venous, arterial, diabetic neuropathic, and hypertensive ulcers. It provides information on: 1. The causes, risk factors, signs and symptoms, investigations and management for each type of ulcer. 2. Venous ulcers are the most common type, caused by venous insufficiency and reflux, and are typically treated with compression therapy and dressings. 3. Arterial ulcers are caused by peripheral arterial disease and present with dry necrotic wounds, often over bony prominences of the feet. Revascularization may be required for healing. 4. Diabetic and neuropathic ulcers occur due to loss of sensation from









































































