This document provides an overview of skin ulcers, including their epidemiology, classification, characteristics, specific types, management, and complications. Ulcers can be classified as either specific (caused by infections like tuberculosis) or non-specific (including traumatic, vascular, and neuropathic ulcers). Management involves taking a thorough history, examining the ulcer characteristics, investigating potential underlying causes, treating any identified conditions, regularly dressing the wound, and educating patients on prevention of recurrence. Complications can include infection, osteomyelitis, contractures, and non-healing if not properly managed.
Outline
• Introduction
• Epidemiology
•Characteristics of an ulcer
• Classification
• Specific ulcers
• Non-Specific Ulcers
• Management
– History
– Examination
– Investigation
– Treatment
• Complications
• Follow-up
• Conclusion
• References
3.
Introduction
• An ulceris the loss of continuity of the surface
epithelium.
• The underlying tissues may be affected.
• There are several causes of an ulcer but
necrosis or death of the cells is the immediate
cause
4.
Epidemiology
• It accountsfor about 25-30% of general plastic
surgery visits in industrialized countries
• In developing countries it constitutes about
35-40% of plastic surgery clinic
• About 80% of the ulcers are in the lower third
of the leg
• In the industrialized countries the commonest
cause are venous, diabetic trauma
• In developing countries the common causes
are infection, trauma, venous
5.
Characteristics of anulcer
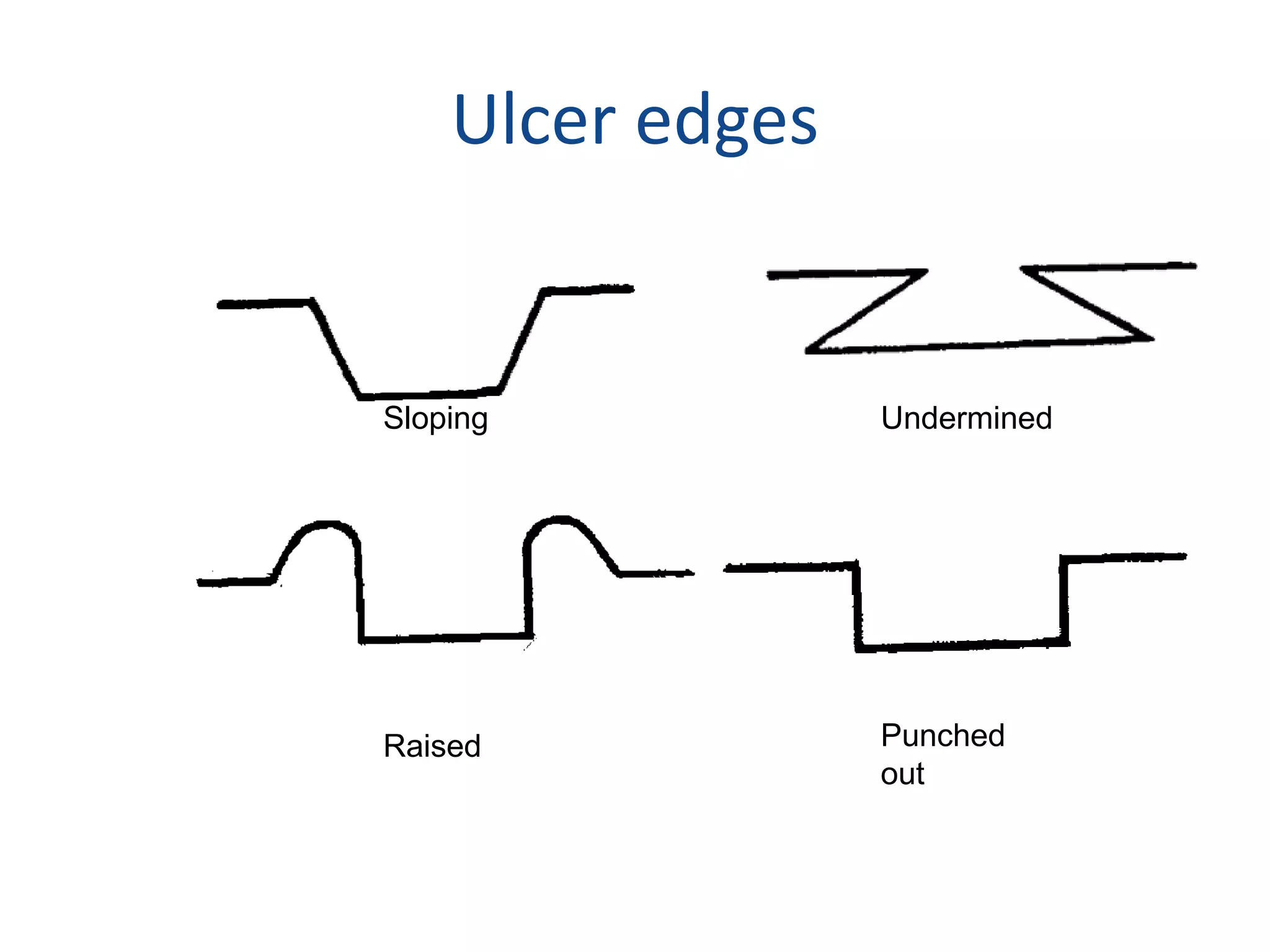
EDGE
It is where the healthy skin (epithelium)begins.
• Sloping in a non-specific ulcers
• Undermined in a Tuberculous ulcers
• Raised in Malignant
• Punched out in syphilis
Specific Ulcers
TROPICAL ULCER
•Acute ulcerative cutaneous lesion caused
synergistically by the anaerobic
Fusobacteria(Bacteriodes fusiformis) and the
aerobic Borrelia vincenti.
• Starts as a Painful septic blister which sloughs
to form an ulcer.
Pathology
• Painful septicblister or vesicle containing sero-
sanguinous fluid surrounded by oedematous
inflamed skin
• Ruptures after a few days to expose a foul-smelling,
ragged, yellowish brown, grey or black slough of the
skin and subcutaneous tissues
• Lymphadenitis or lymphangitis
• Can affect deeper structures such as muscles and
tendons causing them too to slough off
16.
• Blood vessels,if affected get thrombosed.
• Gangrene may result if it is an end artery.
• Bones------- periostitis.
• The slough with time liquefies, discharges
offensive pus and separates.
• A circular ulcer about 4-l0cm in diameter then
forms
17.
TB ULCER
• Irregularoutline and the edges are thin, blue
and undermined
• Floor is covered with pale granulations and
the discharge is thin and watery. The base is
soft.
• There may be satellite sinuses and enlarged
lymph nodes.
• There may be a tuberculous focus in the lung
or bone.
18.
BURULI ULCER
• Mycobacteriumulcerans
• Temperatures lower than central body
temperature- 30-320C.
• This toxin is thought to be responsible for the
necrosis of the dermis and subcutaneous
tissues seen in typical lesions.
ULCERATIVE
• Necrotic stage;typical white central plug of
necrotic fat, if not interfered with forms a
necrotic slough.
• Organising Stage: the slough separates leaving
an ulcer with edematous base and
undermined edges.
• Healing Stage: the ulcer at this stage is fairly
clean and healing starts.
21.
SYPHILITIC (GUMMATOUS) ULCER
•It is now uncommon.
• It follows breakdown of a subcutaneous
gumma especially around the knee.
• It has a serpiginous outline because as it heals
in some parts it spreads in others.
22.
YAWS
• Starts asa small erythematous macule which
becomes an enlarging papule up to 5cm wide.
• The skin often ulcerates and exudes a serous
fluid. It heals spontaneously.
• Ulceration and secondary infection may occur.
• Resembling syphilitic ulcers, they are punched
out with sloughing base.
• They heal spontaneously after a few weeks, the
skin over them often becoming depigmented.
The regional lymph nodes are enlarged
24.
B. Non-Specific Ulcers
Skinulcers go through the following phases.
• 1. Acute or Infective phase:
– Ulcer is painful. The sloughing floor is covered
with purulent discharge in which different types of
bacteria may be identified.
– The edge is sharp and surrounded by damaged
cells. The surrounding skin is oedematous, warm
and tender
25.
• 2. Transitionphase:
– The slough separates, the pus drains, infection
subsides, granulation tissue grows and the floor
becomes clean and red.
– The edge, which is sloping, has a thin bluish-white
layer of young epithelium growing inwards.
– The surrounding skin is slightly hyperaemic or
normal.
26.
• 3. Reparativeor healing phase;
– The ulcer is now painless. The healthy granulation
tissue fills the floor and the epithelium grows from
the edge.
27.
• 4. Chronic,indolent or callous phase:
– Some ulcers may remain unhealthy for a long
time
– The edges are then ragged, the floor greyish or
creamy pink with profuse offensive discharge, and
the surrounding skin warm and oedematous.
MANAGEMENT
HISTORY
• Onset andcourse
• Symptoms
• Medical History
• Family History
• Drug History
• Personal Habits
PHYSICAL EXAM
• General
• Peripheral
neuropathy
• Peripheral pulses
• Regional LNs
30.
2. Clinical Examination
•(a) Ulcer:
• (i) Number:- Multiple ulcers may be due to
Kaposi’s sarcoma, yaws, spherocytosis, ulcerative
colitis or self inflicted injuries
• (ii) Anatomical site: - An ulcer near the medial
malleolus may be venous, traumatic or due to
SCDx
• One in the groin or neck is probably tuberculous.
31.
• (iii) Thesize.
• (iv) The shape; whether round, oval, irregular or
serpiginous (syphilitic).
• (v) Edge:-This is the most important part of the ulcer.
– Sloping edge - non-specific ulcer.
– Raised and everted -malignant ulcer.
– Raised and rolled - rodent ulcer.
– Undermined- tuberculous or Buruli ulcer.
– Punched out – syphilitic or yaws.
32.
• (vi) Floor- whether sloughy and discharging;
clean and pink (healing) or nodular
(malignant). Type of discharge is also noted.
• (vii) Base - whether slightly indurated as in
chronic nonspecific ulcer or indurated and
fixed as in carcinoma or callous non-specific
ulcer.
33.
• (viii) Thesurrounding skin - whether it is inflamed or
pigmented.
• (ix) The state of local circulation - presence of dilated
veins. Oedema of tissues, temperature and colour
of skin or toe nails.
• (x) State of innervation - any loss of sensation or
motor function.
• (xii) Regional lymph nodes - this is important
especially in carcinomatous ulcers. If enlarged,
tender or mobile
TREATMENT (Non-specific ulcers)
•Acute
– Admit, bed rest and elevate affected limb
– Broad-spectrum antibiotics and Antitetanus.
– Wound dressings
– The affected limb is splinted in the position of function to
prevent formation of contracture.
– Physiotherapy is started early to prevent wastage of muscle
and contractures.
– Once the ulcer becomes healthy, it is covered appropriately
• Chronic
– Wide excision
– Skin graft/flap
Follow up
• 1.the patient is advised to protect the affected
skin for example- the legs and feet by wearing
comfortable socks and shoes.
• 2. Farmers are advised to wear protective
clothing and boots.
• 3. Advised about proper foot hygiene.
• 4. Where there is extensive scarring, the patient
is advised to continue wearing medical stocking
or crepe bandage.
• 5. To seek prompt attention for any abrasion or
laceration to the affected skin.
43.
Conclusion
• Management ofpatients with skin ulcers has
to be multidisciplinary.
• Should include detailed history, physical
examination, investigations, basic and newer
treatment modalities.
• While educating patients on issues of correct
skin care and the importance of seeking early
medical advice.
44.
References
• O. Amir,A. Liu, and A. L. S. Chang, “Stratification of highest-risk patients
with chronic skin ulcers in a Stanford retrospective cohort includes
diabetes, need for systemic antibiotics, and albumin levels,” Ulcers, vol.
2012, Article ID 767861, 7 pages, 2012.
• C. K. Sen, G. M. Gordillo, S. Roy et al., “Human skin wounds: a major and
snowballing threat to public health and the economy,” Wound Repair and
Regeneration, vol. 17, no. 6, pp. 763–771, 2009.
• Oluwatosin OM. Wounds and Wound Healing.In Oluwatosin OM ed.
Methods of Repair.Abeokuta.Sagaf Publishers 2007. 6thedition.





























![TREATMENT (Specific ulcers)
• Acute
– Tropical
– Admit
– Antibiotics
– Sloughectomy [surgical or non-operative].TT,SPLINTING,PHYSIO
• Chronic
– Tuberculous
– Antituberculous regimen
– Syphilitic
– Penicillin
– Buruli
– Medical
– Antituberculous drug
– Heat treatment
– Surgical
– Pre-ulcerative –nodulectomy, wide excision
– Ulcerative –debridement, split skin graft/flap](https://image.slidesharecdn.com/skinulcersoverview-210206041202/75/Skin-Ulcers-Overview-ppt-36-2048.jpg)