Downloaded 126 times











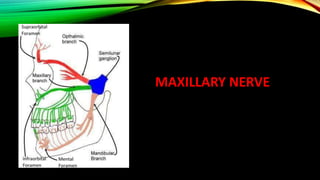




























The document provides a detailed overview of the trigeminal nerve, its anatomy, and functions, including the sensory and motor roots and their corresponding branches (ophthalmic, maxillary, and mandibular divisions). It describes the trigeminal ganglion's relationships with surrounding structures and the various sensory and motor functions each division serves. Additionally, it explores the associated branches, such as nasociliary and maxillary nerves, and their anatomical pathways and functions in innervating facial structures.























































































