Downloaded 507 times
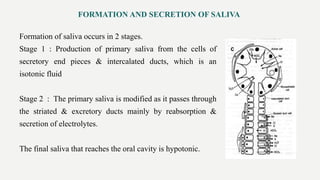
![Salivary flow
• The average person produces approximately 0.5 L – 1.5 L per day
Unstimulated Flow (resting salivary flow―no external stimulus)
• Typically 0.2 mL – 0.3 mL per minute
Stimulated Flow (response to a stimulus, usually taste, chewing, or
medication [eg, at mealtime])
• Typically 1.5 mL – 2 mL per minute](https://image.slidesharecdn.com/saliva-diagnostictool-180713035604/85/Saliva-as-a-Diagnostic-Tool-5-320.jpg)
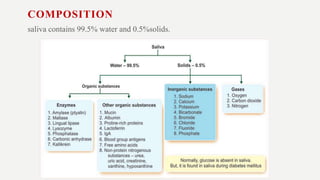


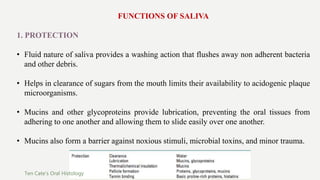
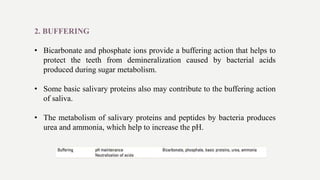
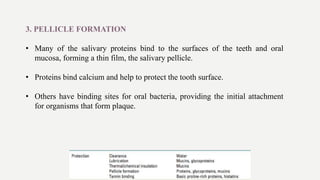

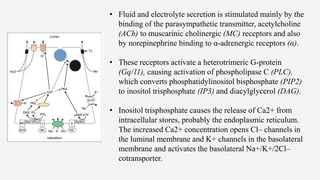
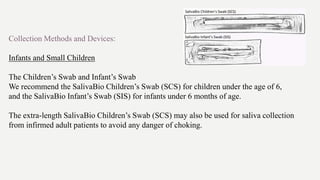




This document discusses saliva as a diagnostic fluid. It defines saliva and describes its general properties, composition, formation, and functions. Methods for collecting saliva are provided for adults, children, and infants. Advantages of saliva analysis include its noninvasive nature, low cost, and applicability for screening large populations. Limitations relate to variability in salivary markers based on collection method and flow rate. The document outlines analysis of saliva for diagnosing conditions like Sjogren's syndrome based on changes in immunoglobulin and protein levels.











































![saliva [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/salivaautosavedautosaved-220908033511-b60e738f-thumbnail.jpg?width=640&height=640&fit=bounds)











































