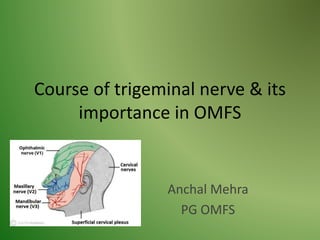
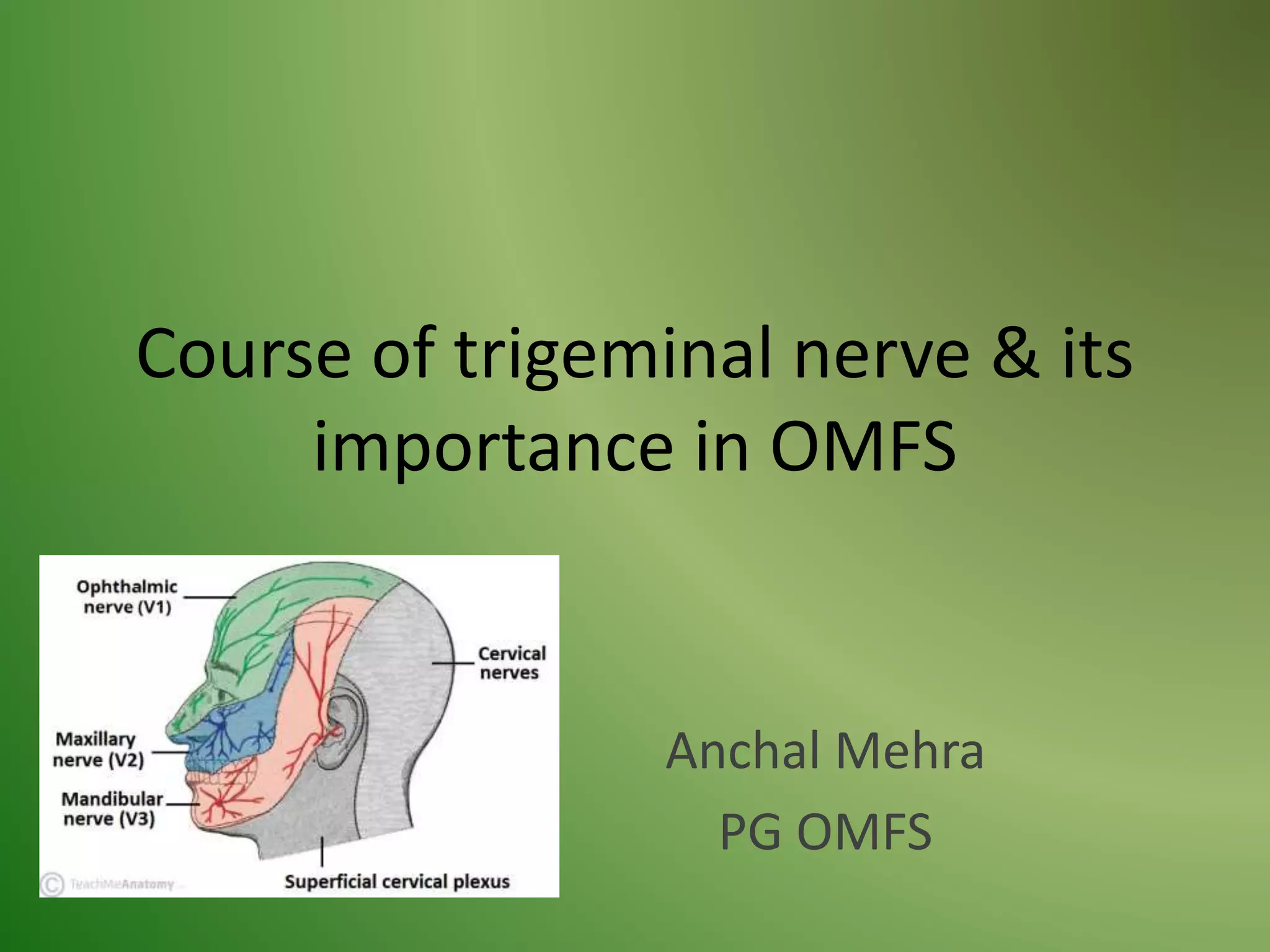
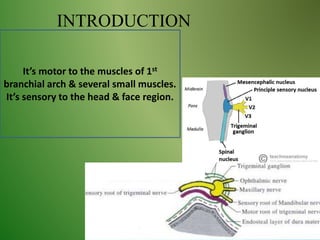
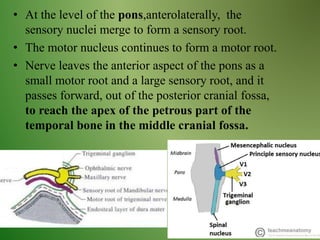
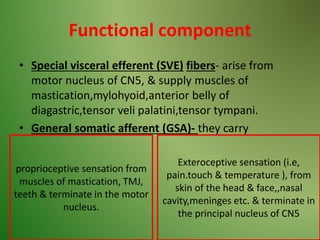
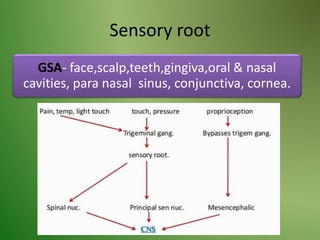
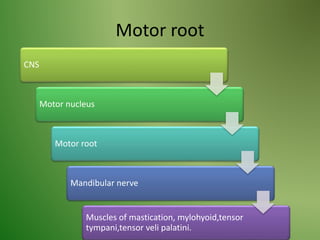
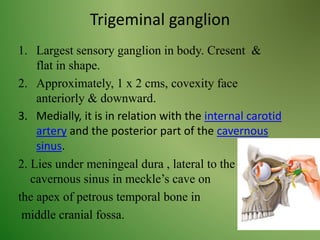
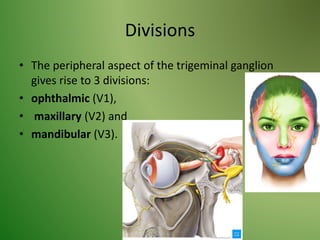
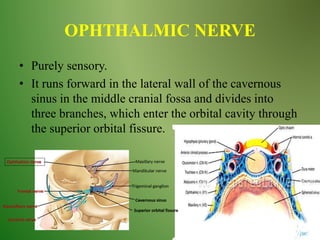
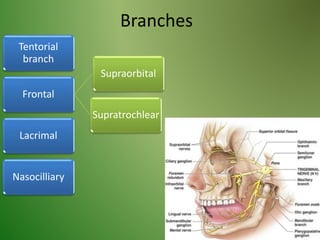
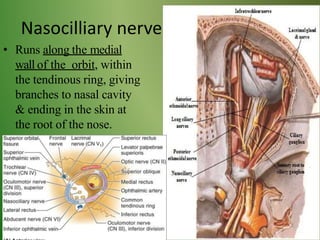
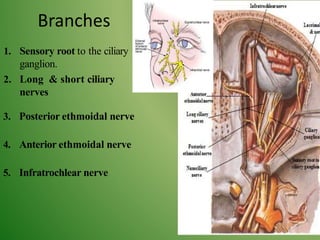
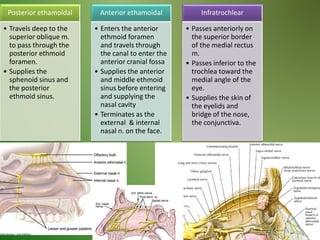
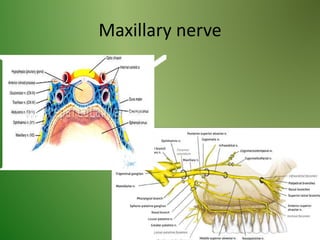
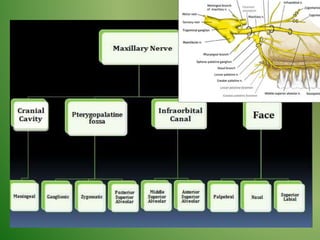
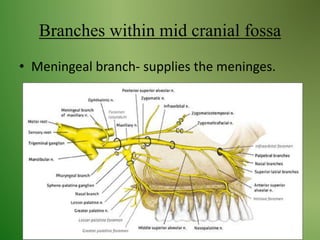
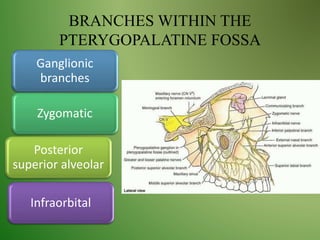
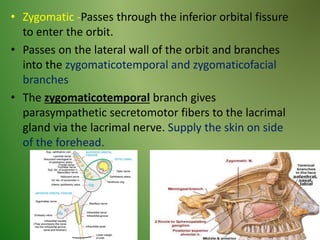
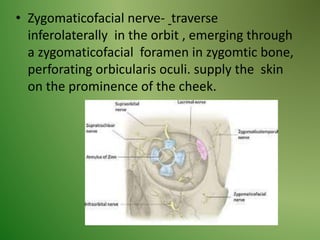
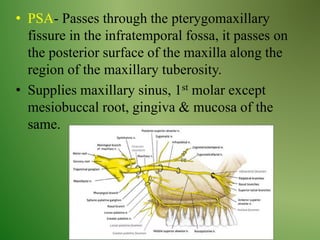
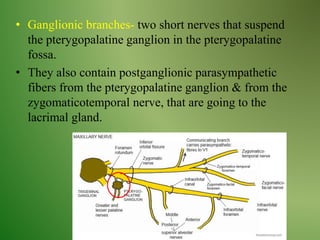
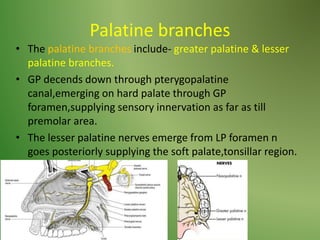
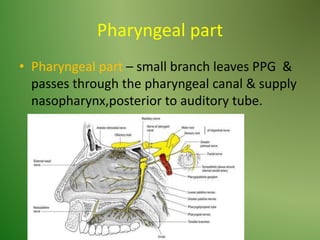
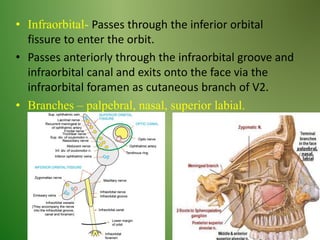
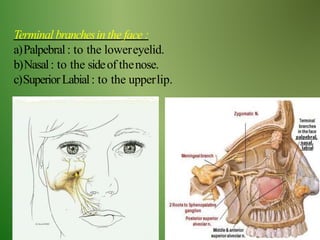
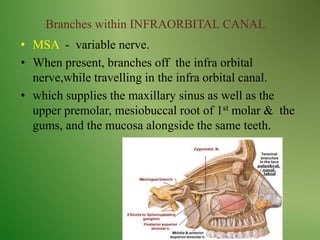
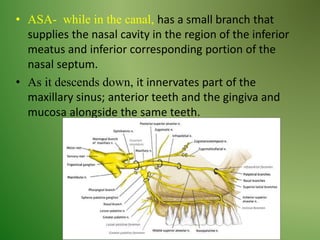
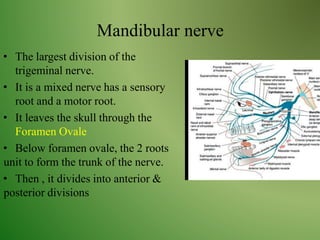
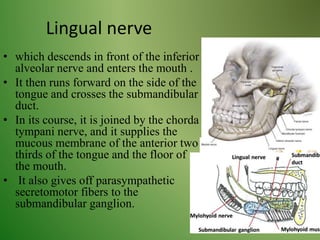
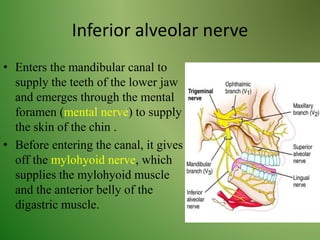
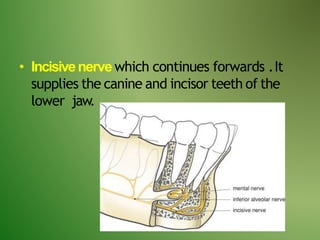
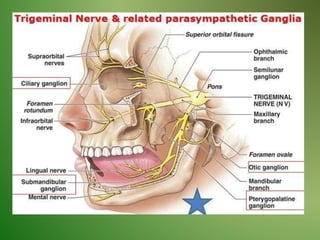
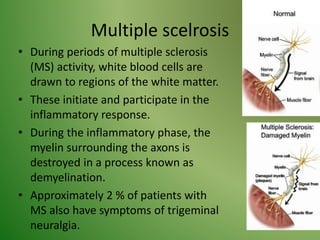
The document provides an overview of the anatomy and clinical importance of the trigeminal nerve (CN V). It discusses the motor and sensory components and divisions of the nerve. Key points include that CN V has three divisions - ophthalmic, maxillary, and mandibular. It summarizes branches of each division and their functions. The document also covers clinical examination techniques for CN V and related pathologies like trigeminal neuralgia.