Downloaded 87 times


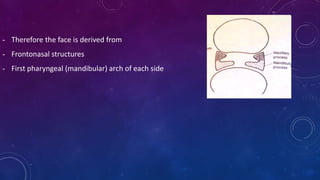
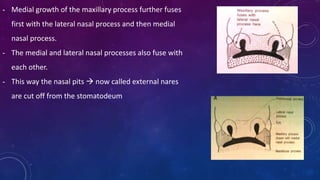


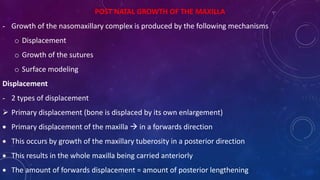






The document details the embryological development of the human face, starting from the 4th week of intrauterine life, including the formation of key structures like the maxilla, nasal processes, and anatomy of the lips. It also discusses mechanisms for postnatal growth of the maxilla and outlines several clinical considerations related to facial development anomalies such as hare lip and macrostomia. The growth processes involved include displacement, growth at sutures, and surface remodeling, highlighting how these factors contribute to the formation and size change of facial structures.





































![Growth & development of maxilla & mandible.ppt [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/growthdevelopmentofmaxillamandible-180610064645-thumbnail.jpg?width=640&height=640&fit=bounds)
































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















