
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Trigeminal nerve final
Similar to Trigeminal nerve final (20)
Recently uploaded
Recently uploaded (20)
Trigeminal nerve final
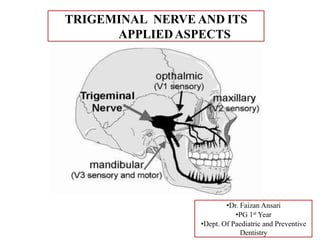
- 1. TRIGEMINAL NERVE AND ITS APPLIEDASPECTS •Dr. Faizan Ansari •PG 1st Year •Dept. Of Paediatric and Preventive Dentistry
- 2. CONTENTS 2 1. Introduction 2. Trigeminal Nerve 3. Trigeminal Nuclei 4. Functional Components 5. Course and Distribution 6. Trigeminal Ganglion 7. Divisions of Trigeminal Nerve 8. AppliedAnatomy 9. Conclusion 10. References
- 3. INTRODUCTION CRANIALNERVES: • Cranial nerves are the nerves that emerge directly from the brain. • Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck. • 12 pairs of cranial nerves as follows: 1. Olfactory nerve 2. Optic nerve 3. Occulomotor nerve 4. Trochlear nerve 5. Trigeminal nerve 6. Abducens nerve • The cranial nerves are considered as a component of the peripheral nervous system. 7. Facial nerve 8. Vestibulocochlear nerve 9. Glossopharyngeal nerve 10. Vagus nerve 11. Accessory nerve 12. Hypoglossal nerve 3
- 4. CRANIAL NERVES ( I – XII) 4
- 5. • The trigeminal nerve is so called because of its three main divisions i.e. the Ophthalmic, Maxillary & Mandibular nerves. • It is the largest of the cranial nerves. • It is the fifth cranial nerve. • It is a mixed nerve. • It is sensory to the greater part of the scalp, the teeth and the oral and nasal cavities. • Motor supply is to the muscles of mastication. Proprioceptive nerve fibres arise from the masticatory and extra-ocular muscles. TRIGEMINAL NERVE
- 6. MOTOR ROOT • It arises separately from the sensory root in the motor nucleus of pons. At the semilunar ganglion it passes inferolaterally under the ganglion towards foramen ovale, through which it leaves the middle cranial fossa along with the mandibular division. • After it exits the skull, it unites with the sensory root and forms a single nerve trunk. • It supplies the following muscles: i. Muscles of mastication ii. Mylohyoid iii. Anterior belly of the diagastric iv. Tensor tympani v. Tensor veli palatini
- 7. SENSORY ROOT •The fibres of the sensory root arise from the cells of the trigeminal ganglion. •The branches of the unipolar cells of the trigeminal ganglion are divided into central and peripheral branches. •The central branches leave the concave surface to enter the pons. •The peripheral branches are grouped to form the ophthalmic and maxillary nerves and sensory part of the mandibular nerve.
- 9. THE TRIGEMINAL GANGLION • Sensory root fibres of the trigeminal nerve comprise the central process of cells located in the trigeminal ganglion. • 2 ganglion, one inervating each side of face located in meckel’s cavity on the anterior surface of the petrous portion of temporal bone measures approx. 1.0 x 2.0 cm. • It lies at depth of 4.5-5 cm from the lateral aspect of the head near the posterior part of the zygomatic arch. • It is cresentic or semilunar in shape. Medially it is related to I.C.A & cavernous sinus, inferiorly with the motor root and the greater petrosal nerve & the apex of the petrous temporal bone and foramen lacerum. • Blood supply to the ganglion is through the ganglionic branches of the ICA & the accessory meningeal artery which enters through the foramen ovale.
- 10. 28 TRIGEMINAL GANGLION LOCATION OF THE TRIGEMINAL GANGLION: At the apex of the petrous temporal bone on the floor of middle cranial fossa.
- 11. Various nuclei associated with the fifth nerve are situated within the pons. They are: 1. Motor nucleus 2. Sensory nucleus 3. Mesencephalic nucleus 4. Spinal nucleus The 3 Main divisions of the trigeminal nerve are : (V1) Opthalmic division. (V2) Maxillary division. (V3) Mandibular division.
- 13. OPTHALMIC NERVE •It is the superior division of the V nerve & is the smallest. •Leaves the cranium and enters the orbit through superior orbital fissure. •It is wholly sensory. •It has 3 branches. All 3 of them pass through the superior orbital fissure into the orbit. They are; 1. Lacrimal nerve 2. Frontal nerve 3. Nasociliary nerve
- 14. COURSE: Emerges from the Trigeminal ganglion Lateral wall of the Cavernous sinus Gives off 3 branches in the anterior part of the Cavernoussinus Lacrimal, Nasociliary and Frontal Superior Orbital fissure ORBIT 14
- 15. 15
- 16. 1. Lacrimal nerve: It is the smallest. It supplies the lacrimal gland & the conjuntiva. It pierces the orbital septum and ends in the skin of the upper eyelid. 2. Frontal nerve: •It is the largest branch & appears to be the direct continuation of the ophthalmic division. It enters the orbit through the Superior Orbital Fissure and divides into 2 branches. i. The supra orbital branch: It is larger & more laterally placed. It supplies the skin of the forehead & scalp as far back as the vertex. It also supplies the mucous membrane of the frontal sinus & pericranium. ii. The supra trochlear branch: It is smaller & more medially placed. It curves upward on the forehead, close to the bone. It supplies the skin of the upper eyelid & lower part of the forehead.
- 17. 3. Nasociliary nerve: It is intermediate in size & runs more deeply. Its branches are divided as following: i. Branches in the Orbit ii. Branches in the Nasal cavity iii. Branches on the face (I) Branches in the Orbit: a. Long root of the ciliary ganglion: It is sensory & passes through the ganglion without synapsing and supplies the eyeball. b. Long ciliary nerve: Supplies the Iris & Cornea. c. Posterior ethmoidal nerve: It enters the posterior ethmoidal canal & supplies to the mucous membrane lining of the Posterior Ethmoidal & Sphenoidal paranasal air cells.
- 18. d. Anterior ethmoidal nerve: It supplies to the anterior ethmoidal & frontal paranasal air cells. In the upper part of the nasal cavity, it further divides into: Internal nasal branches: It has medial/septal branches to the septal membrane. It also has lateral branches, which supply the nasal conchae & the anterior nasal wall. External nasal branches: It supplies the skin on the tip & ala of the nose.
- 19. (II) Branches in the nasal cavity: •The branches arising here supply the mucous membrane of the nasal cavity. (III) Terminal branches on the face: •They supply sensory nerves to the skin of the medial parts of the both eyelids, the lacrimal sac. They also supply skin on the bridge of the nose.
- 20. MAXILLARY NERVE •This is the second & intermediate division of the trigeminal nerve. •It is wholly sensory. Course: It begins at the middle of the trigeminal ganglion as a flattened, plexiform band, passes horizontally forwards along the lateral wall of the cavernous sinus. It leaves the skull through the foramen rotundum & becomes more cylindrical & firmer in texture. It crosses the upper part of the pterygopalatine fossa, inclines laterally on the posterior part of the orbital process of the maxilla & enters the orbit through the inferior orbital fissure. It is now termed as the infra orbital nerve. It passes through the infra orbital groove & canal in the floor of the orbit & appears on the face through the infra orbital foramen.
- 22. BRANCHES Within cranium In pterygopalatinefossa In infraorbitalcanal On face MAXILLARY NERVE Middle meningeal nerve • Inferior palpebral • Lateral nasal • Superior labial • MSA (middle superior alveolar nerve) • ASA (anterior superior alveolar nerve) Zygomatic PSA (posterior superior alveolar) Pterygopalatine •Zygomatico temporal •Zygomatico facial •Orbital •Nasal •Palatine •Pharyngeal 22
- 23. I. Branch given off on the cranium: 1. Meningeal branch: It is given off near the foramen rotundum. It supplies the duramater of the anterior & middle cranial fossae. II. Branches in the pterygopalatine fossa: 1. The ganglionic branches: They connect the maxillary nerve to the pterygopalatine ganglion. They contain secretomotor fibres to the lacrimal gland. They provide sensory fibres to the orbital periosteum & mucous membrane of the nose, palate & pharynx. 2. The zygomatic nerve: It arises in the pterygopalatine fossa from the maxillary nerve and travels anteriorly, entering through the inferior orbital fissure where it divides into 2 branches. The Zygomaticofacial nerve perforates the facial surfaces & supplies the skin over the zygomatic bone.
- 24. The Zygomaticotemporal nerve perforates the temporal surface of the zygomatic bone, pierces the temporalis fascia & supplies the skin over the anterior temporal fossa region. 3. Posterior superior alveolar nerve: It begins in the pterygopalatine fossa but divides into 3 branches which emerge through the pterygomaxillary fissure. • 2 branches enter the posterior wall of the maxilla above the tuberosity & supply the 3 molar teeth (except the mesiobuccal root of first molar). • The third branch pierces the buccinator & supplies the adjoining part of the gingiva & cheek along the buccal side of the upper molar teeth.
- 25. III. Branches in the Infraorbital canal( Infraorbital nerve) 1. Middle superior alveolar nerve: It arises from the Infra orbital nerve & runs downwards & forwards along the infraorbital groove along the lateral wall of the maxillary sinus. It divides into branches which supply the maxillary premolars & mesiobuccal root of the first molar teeth. 2. Anterior superior alveolar nerve: It also arises in the infraorbital canal near the mid point. It runs in the anterior wall of the maxillary antrum. It runs inferiorly & divides into the branches, which supply the canine & incisors. A nasal branch from this nerve, given off from the superior dental plexus supplies the mucous membrane of the anterior part of the lateral wall & floor of the nasal cavity. It ends in the nasal septum.
- 27. IV. Branches given on the face: i. The palpebral branches: They arise deep to the orbicularis oculi & pierce the muscle, supplying the skin over the lower eyelid & lateral angle of the eye along with the Zygomaticofacial & Facial nerves. ii. The nasal branches: They supply the skin of the nose & tip of the nasal septum & join the External nasal branch of the anterior ethmoidal nerve. iii. The superior labial branches: These are large & numerous. They supply the skin over the anterior part of cheek & the upper lip including the mucous membrane & glands. They are joined labial by the facial nerve & form the infraorbital plexus.
- 29. SPHENOPALATINEPTERYGOPALATINE GANGLION •It is the largest of the peripheral ganglia. •It is associated with the greater petrosal nerve. ( Functionally it is part of the Facial nerve). •It acts as a relay station between the superior salivatory nucleus in the pons and the lacrimal gland & mucous & serous glands of the palate, nose & paranasal sinuses. •It lies in the pterygopalatine fossa, suspended from the maxillary division of the trigeminal nerve by 2 roots just in front of the opening of the pterygoid canal. •Branches arise from the maxillary nerve through its ganglionic branches. •They do not establish any sympathetic connections with cells. The branches are: -
- 30. The branches of the Pterygopalatine ganglion are:- I. Orbital branches. II. Palatine branches. Anterior/greater palatine Middle palatine Posterior palatine III. Nasal branches: Posterior superior lateral Nasopalatine/Sphenopalatine IV. Pharyngeal branch.
- 32. 1. Orbital branches: •They are made up of afferent fibres & convey sensory impulses from the periosteum of the orbit. Others supply the mucous membrane of the Posterior ethmoidal & sphenoidal air cells. 2. Palatine branches: •They are distributed to the roof of the mouth, soft palate, tonsil & lining membrane of the nasal cavity. It gives of three branches. They are:-
- 33. i. Greater palatine nerve: It emerges from the foramen medial to the 3rd molar, continues forward splitting into number of branches. It is sensory to the mucosa of the hard palate & palatal gingiva. ii. Middle palatine nerve: This nerve emerges from a small foramen in the medial aspect of the pyramidal part of the palatine bone. Sensory supply is to the mucous membrane of the soft palate. iii. Posterior palatine nerve: It emerges from a foramen slightly lateral to the median palatine nerve. It contains sensory & secretomotor fibres to the mucous membrane of the Tonsillar area.
- 35. 3. Nasal branches: Posterior superior lateral nerves: They supply the posterior part of the nasal conchae. Nasopalatine (Sphenopalatine) nerve: It passes downwards & forwards between the periosteum & mucous membrane in the region of the vomer, continues downwards & forwards, reaches the floor of the nasal cavity. Descends into the incisal canal to appear in the anterior part of the hard palate & supplies the mucous membrane of the premaxilla. 4. Pharyngeal branches: This branch supplies sensory & secretory fibers to the mucous membrane of the nasopharynx. It arises from the posterior part of the pterygopalatine ganglion and passes through the palatovaginal canal along with the pharyngeal branch of the maxillary artery.
- 36. MANDIBULAR NERVE •It is the third & largest division of the trigeminal nerve. •It is made up of 2 roots: a large sensory root which proceeds from the lateral part of the trigeminal ganglion & almost immediately emerges out through the foramen ovale & a small motor root which passes below the ganglion & unites with the sensory root just outside the foramen. •Immediately beyond the junction of the 2 roots, the nerve sends off the meningeal branch & the nerve to the medial pterygoid. Now the main trunk divides into a small anterior & a large posterior trunk. •As it descends from the foramen, the mandibular nerve lies at a distance of 4 cm from the surface & a little in front of the neck of the mandible.
- 38. The branches of the Mandibular nerve:- I. Branches of the undivided nerve: i. Meningeal branch/nervus spinosus. ii. Nerve to the medial pterygoid II. Branches of the divided nerve: (A) Anterior division: (B) Posterior division: 1. Auriculotemporal nerve 2.Lingual nerve 3.Inferior alveolar nerve 1.Buccal nerve 2.Massetric nerve 3.Deep temporal nerve 4.Nerve to the lateral pterygoid.
- 39. BRANCHES OF THE UNDIVIDED NERVE 1. Meningeal nerve: • It enters the skull through the foramen spinosum along with MMA. • It has anterior & posterior divisions that supply the dura of the middle & anterior cranial fossae. 2. Nerve to the medial pterygoid: • It is a slender branch that supplies to the deep surface of the muscle. • It also gives 1-2 filaments to the tensor tympani & the tensor veli palati muscles.
- 41. BRANCHES OF THE DIVIDED NERVE I. Anterior division 1. The buccal nerve: •It passes between the 2 heads of the lateral pterygoid & descends beneath or through the temporalis. It emerges from under cover of the ramus & anterior border of the masseter & unites with the buccal branches of the facial nerve. •It supplies the skin over the anterior part of the buccinator & mucous membrane lining the buccal surface of the gum.
- 42. 2. The massetric nerve: • Passes laterally above the lateral pterygoid in front of the TMJ & behind the tendon of temporalis. • It passes through the mandibular notch to sink into the masseter muscle. • It also gives a branch to the TMJ. 3. The deep temporal nerves: •They are 2 in number. •They pass above the upper head of the lateral pterygoid, turn above the infra temporal crest & sink into the deep part of the temporalis muscle. 4. The nerve to the lateral pterygoid. •These are 2 in number; one supplying each muscle head.
- 44. II. Posterior Division 1.The Auriculotemporal nerve: Course of the nerve: •The auriculotemporal nerve arises by a medial & lateral roots, that encircle the MMA & unite behind it just below the foramen spinosum. •The united nerve passes backwards, deep to the lateral pterygoid muscle & passes between the sphenomandibular ligament & the neck of the condyle. •It then passes laterally behind the TMJ i.r.t. to the upper part of the parotid. •It emerges from behind the TMJ, ascends posterior to the superficial temporal vessels & crosses the posterior root of the zygomatic arch.
- 45. Branches of the Auriculotemporal nerve: 1. Parotid branches-----secretomotor, vasomotor. 2. Articular branches--- to the TMJ. 3. Auricular branches---to the skin of the helix & tragus. 4. Meatal branches-------Meatus of the tymphanic membrane. 5. Terminal branches-----Scalp over the temporal region.
- 46. 2. Lingual nerve: •It lies between the ramus of the mandible & the muscle in the pterygomandibular space. •It then passes deep to reach the side of the tongue. Here it lies in the lateral lingual sulcus against the deep surface of the mandible on the medial side of the roots of the third molar tooth where it is covered only by mucous membrane of the gum. •From here it passes on to the side of the side of the tongue where it is crosses the styloglossus & runs on the lateral surface of the hyoglossus & deep to the mylohyoid in close relation to the deep part of the submandibular gland & its duct. •It gives off sensory fibres to the tonsil & the mucous membrane of the posterior part of the oral cavity.
- 47. 3. Inferior alveolar nerve: •It is the largest terminal branch of the posterior division of the mandibular nerve. •The nerve descends deep to the lateral pterygoid muscle at the lower border of the muscle, it passes between the sphenomandibular ligament & the ramus to enter the mandibular foramen. •In the canal the nerve runs alongside the inferior alveolar artery as far as the mental foramen where it emerges out & gives off the mental & incisivebranches. •From here the nerve runs in the canal giving of branches to the mandibular teeth as apical fibres & enters the apical foramena of the teeth to supply mainly the pulp as well as the periodontium.
- 48. Branches of the nerve :- 1. Mental nerve: it supplies to the skin of the chin & the mucous membrane as well as the skin of the lower lip. 2. Incisive branch: continues anteriorly from the mental nerve in the body of the mandible to form the incisive plexus & supplies the canine & incisors. 3. Mylohyoid nerve: it is given of before the nerve enters canal & contains both sensory & motor fibres. It pierces the sphenomandibular ligament, descends in a groove in the medial side of the ramus & passes beneath the mylohyoid line supplying the mylohyoid muscle as well as the anterior belly of the digastric.
- 50. Submandibular ganglion: •It is a small ovoid body that is suspended from the lingual nerve above the submandibular salivary gland. •The preganglionic parasympathetic fibres reach the ganglion arising from the superior salivatory nucleus, reaching through the facial, chorda tympani & the lingual nerve. Post ganglionic fibres are conveyed through the submandibular, sublingual & anterior lingual salivary glands. •The sensory nerves reach the ganglion through the lingual nerve. •Sympathetic fibres are derived from the plexus around the facial artery & contain post ganglionic fibres arising in the superior cervical ganglion. •They provide secretomotor fibres to the submandibular & sublingual glands.
- 52. Otic ganglion It is a flattened ovoid body located on the medial side of the undivided nerve. It is situated below the foramen ovale & the MMA. It has 2 main roots:- 1. Parasympathetic preganglionic (secretory) fibres: They arise from the inferior salivatory nucleus. The efferent fibres pass by way of the glossopharyngeal nerve through the jugular canal. Below the canal it passes through the tympanic branch of the glossopharyngeal nerve), passing through the tympanic petrosal branch to reach the ganglion. The postganglionic fibres pass through the auriculotemporal nerve. 2. Sympathetic root: It is made up of the postganglionic fibres that have originated in the superior cervical sympathetic ganglion & the plexus of the MMA. The fibres pass through the ganglion uninterrupted. These fibres reach the parotid through the auriculotemporal nerve. Afferent of sensory nerves come from the parotid through the auriculotemporal nerve.
- 55. 1. Sensory Function: Initially test the sensory branches by lightly touching the face with a piece of cotton wool followed by a blunt pin in three places on each side of the face: i. Around the jawline. ii. On the cheek, and iii. On the forehead.
- 56. 2. Corneal Reflex: •The corneal reflex should also be examined as the sensory supply to the cornea is from this nerve. Do this by lightly touching the cornea with the cotton wool and ask the patient to look away gently. This should cause the patient to shut their eyelids.
- 57. 3. Motor Supply: •To test the motor supply, ask the patient to clench their teeth together, observing and feeling the bulk of the masseter and temporalis muscles. •Ask the patient to then open their mouth against resistance. Feeling of the masseter muscles Feeling of the temporalis muscles
- 58. •Finally perform the jaw jerk on the patient by placing your left index finger on their chin and striking it with a tendon hammer. This should cause slight protrusion of the jaw.
- 59. APPLIED ANATOMY
- 60. 1. TRIGEMINAL NEURALGIA – TICDOULOUREX DEFINITION: •Sudden, usually unilateral, severe, brief, stabbing, lancinating,recurring pain along the distribution of one or more branches of the Trigeminal (vth) nerve. TIC DOULOUREUX •Also Known as Fothergill Disease, Trifacial Neuralgia. •Relatively common •Paroxysm of sudden intense, shocking, stabbing onset of facial pain. •Involves one or more areas of distribution of the Trigeminal nerve. •Maxillary and Mandibular divisions are commonly involved.
- 61. CLINICALFEATURES: Symptoms may include one or more of these features: • Episodes of severe, shooting or jabbing pain that may feel likean electric shock. • Spontaneous attacks of pain or attacks triggered by daily activities like touching the face, chewing, speaking or brushing teeth. • Bouts of pain lasting from a few seconds to several minutes. • Episodes of several attacks lasting a few days, weeks, months or longer – some people have periods when they experience no pain. • Constant burning feeling or aches that may occur before it evolves into the spasm-like pain. • Pain in the areas supplied by the Trigeminal nerve, includingthe cheek, jaw, teeth, gums, lips, or less often the eye and forehead. • Pain affecting one side of the face at a time, though mayrarely affect both sides of the face. • Pain focused in one spot or spread in a widerpattern. • Attacks that become more frequent and intense overtime.
- 62. Local lesions- TRIGGER ZONES •Ophthalmic division : Acute glaucoma -Frontal sinusitis •Maxillary division : Caries -Carcinoma of maxilla -Empyema of maxillary sinus •Mandibular division : Caries -Carcinoma or ulcer of the tongue
- 63. Medication: • Medications used to treat trigeminal neuralgia are those used formany other nerve pain syndromes—drugs originally designed to treat seizures. • These anti-seizure agents suppress or entirely block the pain signals that the trigeminal nerve sends to your brain. • Carbamazepine is to be used as the first-line treatment. • Second line drug treatment is the alternative if carbamazepine is contraindicated or not tolerated. Second-line drug treatments: •Gabapentin , Phenytoin •Lamotrigine •Oxy carbamazepine •Topiramate Baclofen (Antispasmodic) •Tricyclic antidepressants like Amitriptyline and Imipramine
- 64. INJECTION THERAPY • When the medicinal therapy does not provide the relief injection of absolute alcohol and anesthetic solution are used. Injection Of AnestheticSolution: • The nerve may be injected with the 2% Xylocaine Hydrochloride solution to break the pain cycle. • This may be followed by edema at the site of injection and trismus. The relief may last for few weeks to months and injection can be repeated when the pain occurs. Injection Of AbsoluteAlcohol: • Injection of absolute alcohol around the nerve trunk or the ganglion gives good results. • It provides the relief for the period of 6 to 12 months. • The injection are given into the maxillary and mandibular division of trigeminal nerve at the level of the base of skull. • The peripheral alcohol injection are given at the level of infraorbital foramen, mental foramen and inferior alveolar foramen.
- 65. SURGERY • For patients in whom medical therapy has failed, surgery is a viable and effective option. • Among patients who develop TN when younger than 60 years, surgery is the definitive treatment. Surgery exposes the patient to operative risks and the risk of permanent, residual facial numbness and dysesthesias (an abnormal unpleasant sensation felt when touched, caused by damage to peripheral nerves). • The primary complications of surgery include permanent anesthesia over the face or the troubling dysesthetic syndrome of anesthesia dolorosa (an uncommon deafferentation pain that can occur after traumatic or surgical injury to the trigeminal nerve). Three operative strategies now prevail: a) Percutaneous Procedures b) Gamma Knife Surgery (GSK) c) Micro vascular decompression (MVD)
- 66. PERCUTANEOUS SURGERIES • Percutaneous procedures usually can be performed on an outpatient basis under local or brief general anesthesia at acceptable or minimal risk of morbidity. • For these reasons, they are commonly performed in debilitated persons or those older than 65 years. There are 3 types of procedures: i. Percutaneous Radiofrequency Trigeminal Gangliolysis(PRTG) ii. Percutaneous Retrogasserian Glycerol Rhizotomy (PRGR) iii. Percutaneous Balloon Microcompression (PBM).
- 67. PERIPHERAL TRIGEMINAL NERVE BLOCKS, SECTIONING ANDAVULSIONS 1 • Involves injuring the peripheral portions of TN external to skull to provide permanent pain relief. • Indicated in older patients, more than 60 years of age. • Used as the last resort, when all other treatments have failed. 17
- 68. RADIOSURGERY 172 •Several reports have documented the efficacy of Gamma Knife stereotactic radiosurgery for TN. •Because radiosurgery is the least invasive procedure for TN, it is agood treatment option for patients with co-morbidities. •High-risk medical illness or pain refractory to prior surgical procedures.
- 69. 2. TRIGEMINALNEUROPATHY • Often referred to as Trigeminal neuropathic pain. • It is the sensory loss of facial muscles or weakness of the jaw muscles. CAUSES: •SLE •Sjogren’s syndrome •Herpes zoster •Leprosy •Meningioma •Schwanomma, Wallenberg syndrome, Vertebral artery occlusion, Infarction of lateral medulla.
- 70. • SYMPTOMS ipsilateral facial sensory loss, ipsilateral Horner’s syndrome, ipsilateral IX,X,XI palsy, ipsilateral cerebellar ataxia & contralateral sensory loss. TREATMENT - Antiepileptic drugs like Carbamezepine, Phenytoin, Gabapentin. - Tricyclic antidepressants like Amitriptyline andImipramine. - Medications rarely provide complete relief but can reduce the severity of the symptoms. - Counseling of the patient as it is a disease with long termeffects. 17 4
- 71. 3. HERPES ZOSTER OPHTHALMICUS • About 15% of the cases of Herpes zoster (HHV3/Varicella zoster) involvethe trigeminal nerve. • Most frequently affecting nasociliary branch of the Ophthalmicdivision. CLINICALFEATURES: •Pain precedes skin lesion. •Clinical feature is hemifacial unioccular cutaneous lesions Maculopapular rash Vesicle Pustules Crust Permanent scar
- 72. • III, IV,VI th cranial nerve palsy • Progressive proptosis (abnormal protrusion or displacement of an eye or other body part.) • Post herpetic neuralgias • Keratitis, conjunctivitis, scleritis, iritis, anterior uveitis, retinitis. • Without antiviral therapy, 50-70% cases develop ocular complications. Treatment: • Analgesics • Anti depressants • Anti viral therapy for VZV infection • Trigeminal rhizotomy • Stellate ganglion block
- 73. 4. NEUROTROPHIC KERATITIS • Occurs due to partial or complete corneal anaesthesia due to loss of sensory innervation by the Trigeminal nerve. • There is impaired response to corneal microtrauma as a result of impaired regeneration and healing of corneal epithelium. CAUSES: • Bacterial infections – HSV, VZV, Leprosy. • Traumatic vascular nerve injury • Ablation of gasserian ganglion • Chemical burns • Topical anesthetic abuse, • Beta blockers • NSAIDS • Contact lens wear
- 74. SYSTEMIC: • Diabetes mellitus • Stroke • Brainstem hemorrhage • Aneurysm • Congenital TREATMENT: •Mild epithelial defects can be treated with Erythromycin ointment 4-8 times/day. •If corneal ulceration has occurred, smears and cultures are taken to rule out any infections. •If culture is sterile, and no response to ointment is seen, consider a bandage contact lens, tarsorrhaphy, amniotic membrane graft or a conjunctival flap. 184
- 75. 5. RAEDER’S PARATRIGEMINALSYNDROME •Oculosympathetic paresis with pain in distribution of trigeminal Nerve. •Trigeminal hyperasthesia seen in areas supplied by post ganglionic fibers. SIGNS ANDSYMPTOMS: •Pulling pain over the zygomatic region which may radiate behind and below the ear. •Pain presents at morning and recurs at night time. •Wooshing & buzzing sound in the ear. •Numbness over the affected side of face. •Blurred vision. •Unable to bite. •Nostrils appear blocked.
- 76. TREATMENT: • Unless intracranial pathology exists, treatment remains symptomatic. • For the management of associated pain, antispasmodic drug such as Baclofen or anticonvulsants such as Carbamazepine, Gabapentin, Pregabalin and Topiramte may be effective. • Anti-inflammatory agents such as corticosteroids can also be effective, and at times narcotic analgesics such as ergotamines may also be used. • The efficacy of Tricyclic antidepressants (TCAs) has alsobeen demonstrated in some patients. • Vitamin B supplements can be given as adjuvant therapy. • Surgery is not indicated in most patients unless a secondary cause is found which justifies surgicalintervention. 189
- 77. 6. STURGE WEBER SYNDROME/ ENCEPHALO TRIGEMINAL ANGIOMATOSIS •Rare congenital neurological & skin disorder. •Often associated with port-wine stainsof the face, glaucoma, seizures and mental retardation. •It is diagnosed clinically, based on the typical cutaneous, central nervous symptom (CNS), and ocular abnormalities. •Neurological symptoms include: i. Developmental delay or intellectual disability ii. Learning problems iii. Attention deficit hyperactivity disorder (ADHD).
- 78. • Port-wine stains • Macrocephaly • Soft-tissue hypertrophy • Hemiparesis • Visual loss • Ocular manifestations • Hemianopsia (less vision or blindness (anopsia) in half the visual field, usually on one side of the vertical midline) SIGNS AND SYMPTOMS: PORT-WINE STAINS
- 79. TREATMENT: • Medical care includes anticonvulsants for seizure control,symptomatic and prophylactic therapy for headache, glaucoma treatment to reduce intra-optic pressure and laser therapy for port-winestains. • ANTIEPILEPTIC DRUGS: with an efficacy in focal seizures are preferred. The chance of achieving seizure control withmedical treatment varies from patient to patient. • GLAUCOMA MEDICATION: The goal of treatment is tocontrol IOP to prevent Optic nerveinjury. i. Beta-antagonist eye drops – decrease the production of aqueous fluid. ii. Carbonic anhydrase inhibitors – also decrease the productionof aqueous fluid. iii. Adrenergic eye drops and miotic eye drops – promote drainage of aqueous fluid • DYE LASER PHOTOCOAGULATION: Treatment of cutaneous type with Dye Laser photocoagulation has been helpful in reducing the cosmetic blemishes from the cutaneous vascular dilatation. • SURGERY: is desirable in patients who have refractoryseizures, glaucoma, or specific problems related to various disorders associated with Sturge Weber syndrome like Scoliosis.
- 80. CONCLUSION •Trigeminal nerve is a mixed nerve and it mainly supplies the regions of the face, head and neck. •The various techniques of local anesthesia are all directed towards the Trigeminal nerve. Thus, as a Paedodontist one should know thoroughly about the course and distribution of the Trigeminal nerve, to diagnose the pathologies associated with the nerve and their appropriate treatment.
- 81. REFERENCES 1. Gray H. Anatomy of the human body. Lea & Febiger; 1878. 2. Snell RS. Clinical anatomy. Philadelphia: Lippincott Williams & Wilkins; 2004. 3. Chaurasia BD. Human Anatomy: Head and Neck and Brain. 4. Malamed SF. Handbook of local anesthesia. Elsevier Health Sciences; 2004 Jun 8. 5. Monheim LM. Local anesthesia and pain control in dental practice. Mosby; 1965.