Downloaded 118 times
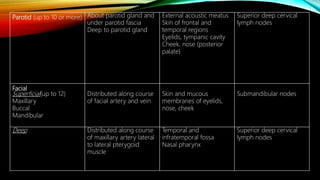
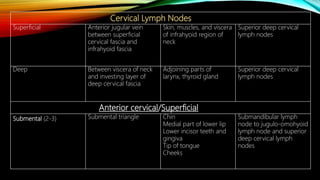

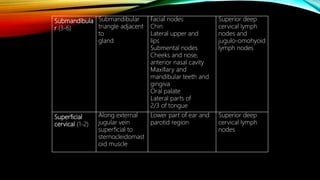

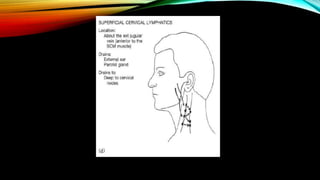
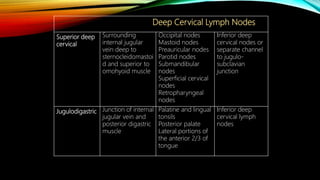
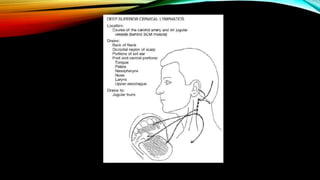
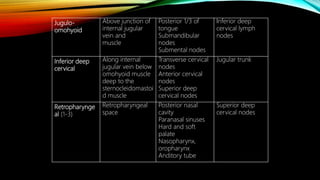
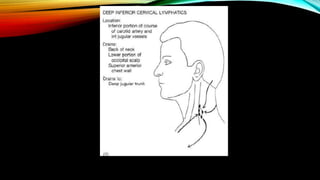
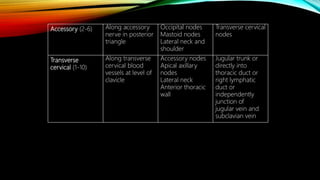

The document discusses the lymphatic system's functions, including fluid recovery, immunity, and lipid absorption, along with its anatomical components such as lymph, lymphatic vessels, and lymphatic organs. It explains the mechanisms of lymph flow, focusing on how lymphatic vessels operate without a central pump and the role of muscles and respiratory actions in aiding circulation. Additionally, it details the classification and locations of various lymph nodes in the body, highlighting their significance in immune defense and fluid transport.























































































