This document provides information on tracheostomy care including:
- The risks of tracheostomy include infection, internal bleeding, and loss of speech.
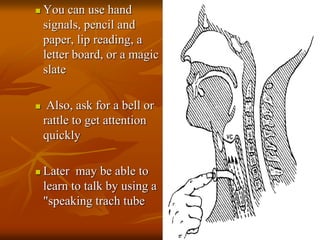
- Pre-op care involves sedation, NPO after 2200 hours, blood tests, consent forms and ensuring communication methods.
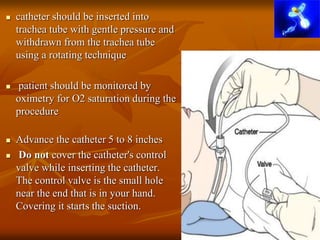
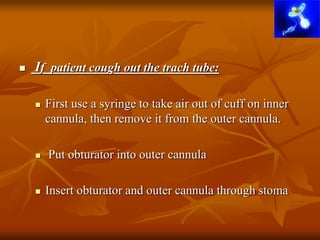
- Post-op care consists of tracheostomy tube cleaning daily, suctioning secretions, monitoring oxygen levels, and giving medications like antibiotics and analgesics.
- Proper tracheostomy care is needed to prevent complications and keep the site infection-free.