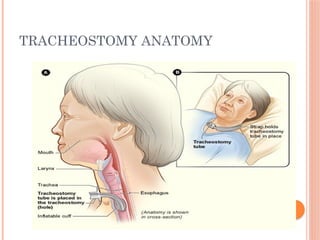
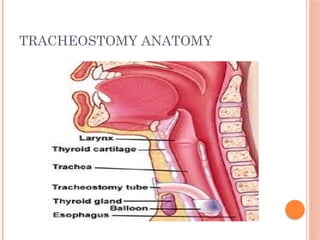
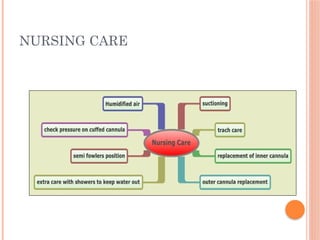
Tracheostomy is a surgical procedure that creates an opening in the trachea to facilitate breathing, often required for patients with severe airway obstruction, respiratory failure, or other medical conditions. Effective care involves regular assessment for complications, proper tube management, and patient education to assist with the adjustment to life with a tracheostomy. Key nursing responsibilities include ensuring the availability of emergency equipment, suctioning, maintaining hygiene at the stoma site, and monitoring for signs of infection and other issues.