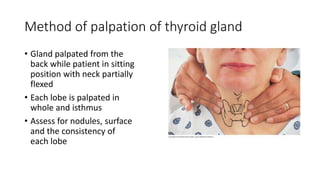
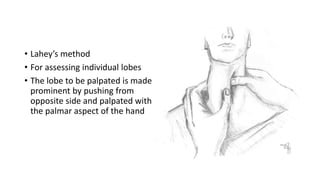
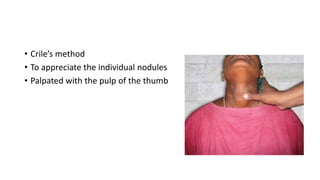
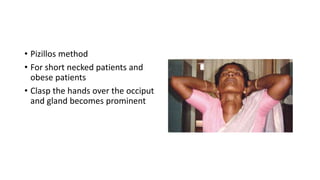
This document outlines the steps for examining a patient's thyroid gland. It details the relevant history to obtain including symptoms, past medical history, and family history. The physical exam involves inspection of the neck and thyroid, palpation of the gland to assess size, consistency, and mobility, and examination of related structures like eyes, skin, and lymph nodes. Tests are described to evaluate for retrosternal extension and tracheal compression. Examination of cardiovascular, neurological and respiratory systems is also recommended given thyroid abnormalities can impact these areas.