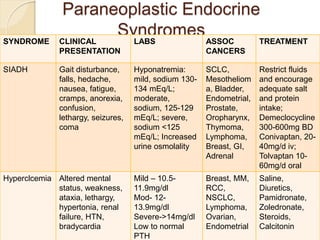
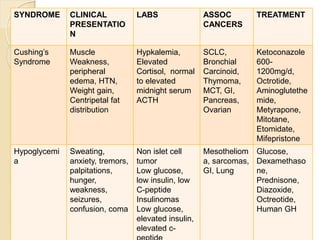
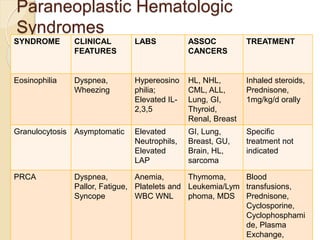
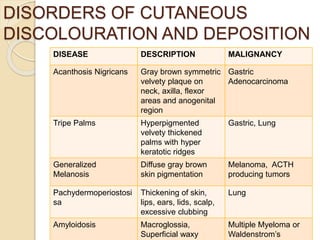
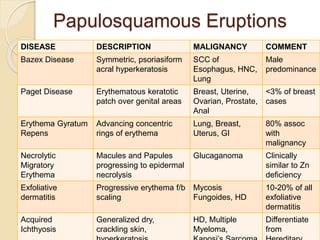
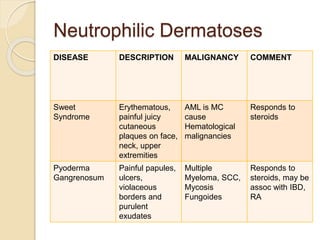
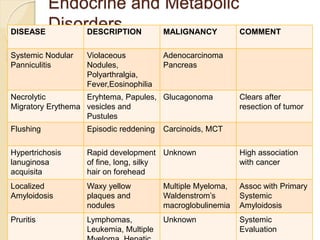
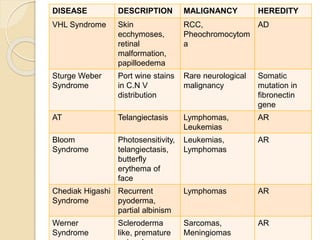
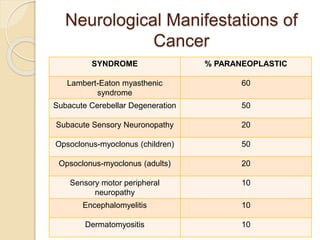
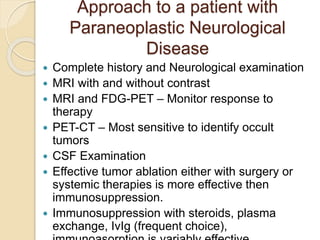
This document discusses paraneoplastic syndromes, which are clinical disorders associated with but not directly caused by malignant tumors. It describes several paraneoplastic endocrine, hematologic, neurological, dermatological, and other syndromes, listing their typical clinical presentations, associated laboratory abnormalities and cancers. It discusses evaluation, treatment and prognosis of these syndromes, noting that successful treatment of the primary tumor often leads to resolution of paraneoplastic symptoms.