Downloaded 1,165 times




![Paradoxical Upgrading Reactions
• Worsening of symptoms during treatment (ie,
paradoxical upgrading reaction [PUR]).
• One definition is the development of enlarging
nodes, new nodes, or a new draining sinus in
patients who have received at least 10 days of
treatment.](https://image.slidesharecdn.com/tubercularlymphadenitismanagement-150227044649-conversion-gate01/85/Tubercular-lymphadenitis-management-57-320.jpg)

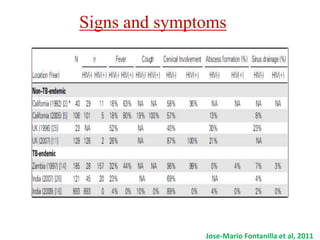
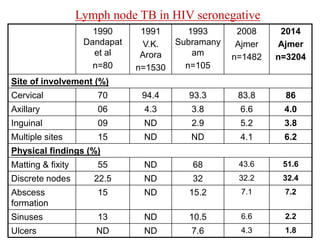
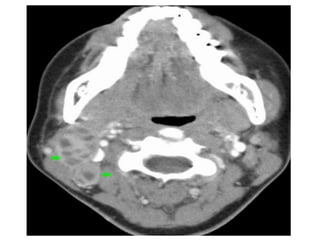
1. Managing lymph node tuberculosis can be challenging as it has varied clinical manifestations and diagnostic challenges. 2. It most commonly involves cervical lymph nodes but can affect nodes throughout the body. 3. Diagnosis may involve imaging like ultrasound, CT, or MRI to identify enlarged or cystic lymph nodes, as well as biopsy to confirm the presence of Mycobacterium tuberculosis. 4. Treatment often requires a multi-drug antibiotic regimen over a prolonged period.














































































