Downloaded 121 times
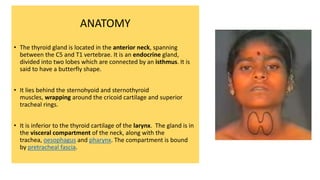













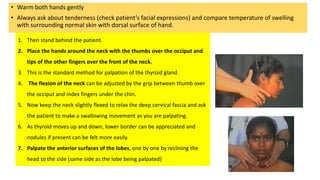







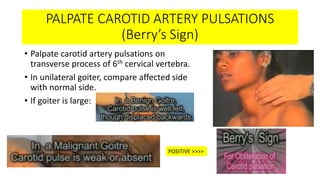
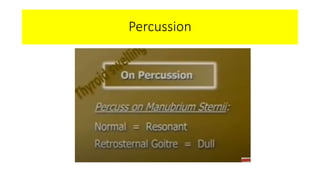

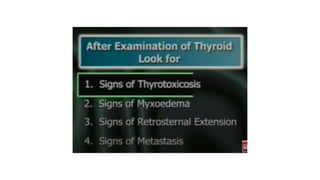


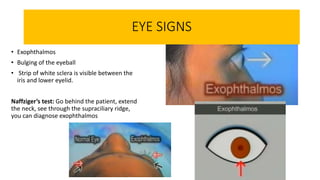





The document provides instructions for examining the thyroid gland. It begins with introducing oneself to the patient and obtaining consent. It describes the anatomy of the thyroid gland and its location. The examination involves inspection of the thyroid from the front and back while palpating and feeling for nodules or irregularities. Signs of hyperthyroidism like eye signs, tremors, and moist skin are also checked. The examination is concluded by checking reflexes and the heart before thanking the patient.















































































