Downloaded 394 times

![Cont’d
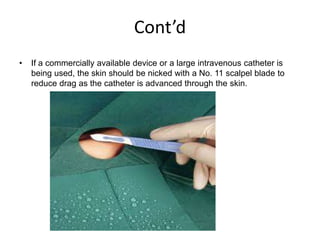
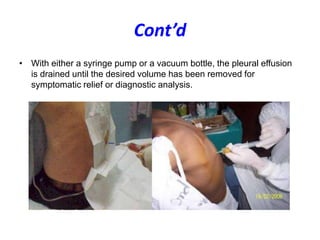
•
•
•
•
•
•
•
•
•
•
Thoracentesis device - This typically consists of an 8-French catheter over
an 18-gauge, 7.5-in. (19-cm) needle with a 3-way stopcock and, ideally, a
self-sealing valve
Self-assembled device, if a thoracentesis device is unavailable - Options
include using an 18-gauge needle or a 12-gauge intravenous (IV) catheter
connected to a 60-mL syringe and then to a stopcock after the needle is
removed from the 60-mL syringe
Injection needle – 22 gauge, 1.5 in. (3.81 cm)
Injection needle – 25 gauge, 1 in. (2.54 cm)
Luer-Lok syringe - 10 mL
Luer-Lok syringe - 5 mL
Luer-Lok syringe - 60 mL
Tubing set with aspiration/discharge device
Antiseptic - Chlorhexidine solution [Hibiclens] is preferred
Lidocaine - 1% or 2% solution, 10-mL ampule](https://image.slidesharecdn.com/thoracocentesis-131012060510-phpapp01/85/Thoracocentesis-13-320.jpg)


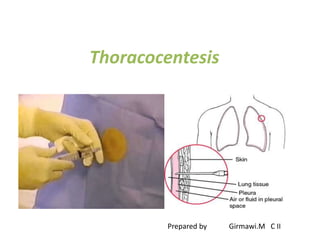
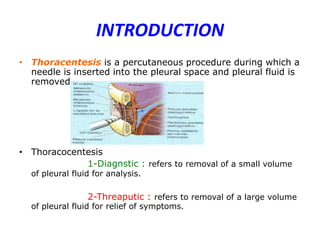
This document provides an overview of thoracentesis, including: - Definition, indications, contraindications, techniques/procedure, materials, and complications of thoracentesis. - Thoracentesis is a procedure to remove fluid from the pleural space, either for diagnostic purposes or to relieve symptoms. It is indicated for large pleural effusions or those requiring diagnostic analysis. - Potential complications include pneumothorax, hemothorax, organ injury, and infection, though minor complications like pain or dry tap are more common. Proper patient preparation, anesthesia, positioning, and sterile technique are emphasized to reduce risks.








































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














