Downloaded 256 times
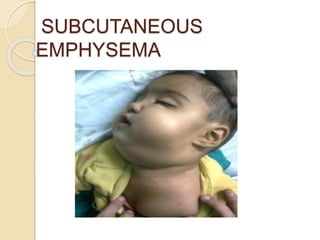
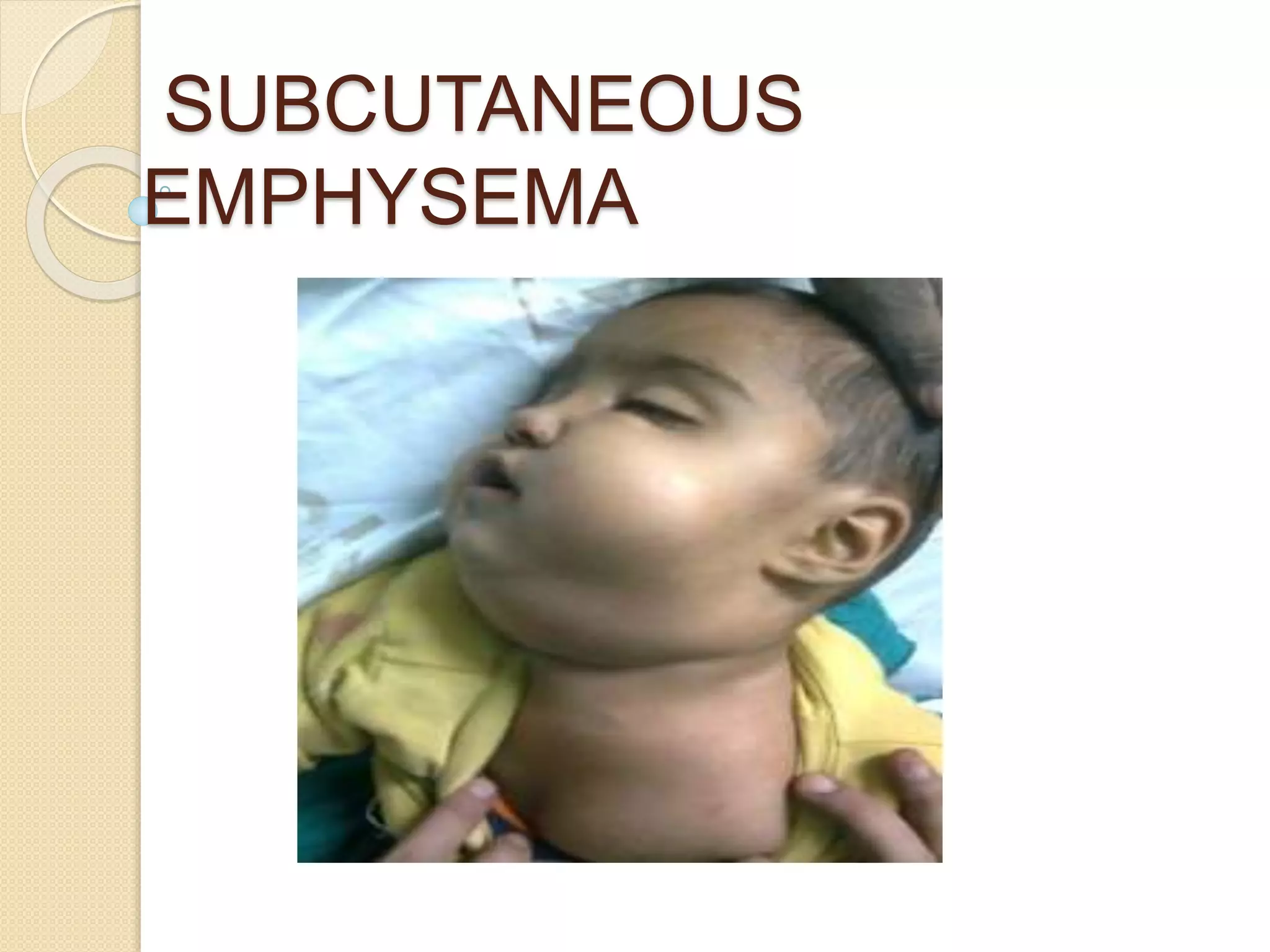
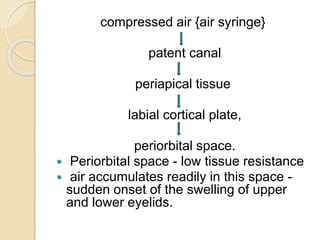
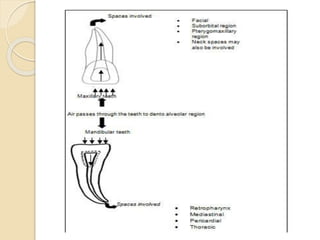
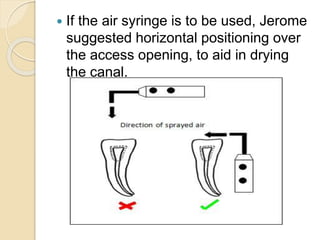

This document discusses subcutaneous emphysema, which occurs when air is introduced into the subcutaneous fascia, causing soft tissue swelling. It can arise during dental procedures when compressed air enters tissues through patent canals or gingival sulci. Common symptoms include localized swelling, crepitus, and discomfort. While usually benign and self-resolving, air can occasionally spread to dangerous areas if not properly managed. Prevention involves avoiding direct air use and instead drying canals with paper points.



![Air leaks in Thoracic Surgery [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/airleaksinthoracicsurgeryauto-saved-230219163120-6180857a-thumbnail.jpg?width=640&height=640&fit=bounds)


































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















