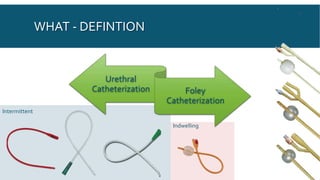
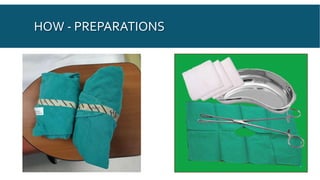
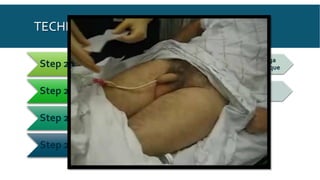
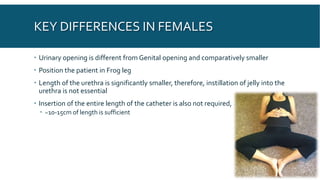
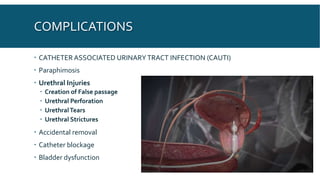
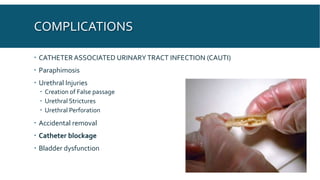
This document provides an overview of urethral catheterization procedures. It defines different types of catheters and discusses catheter anatomy and indications for use. The document outlines the necessary staff and supplies for catheterization and provides a step-by-step description of the catheterization technique for both males and females. Potential complications are reviewed as well as post-procedure care and things to watch out for after catheterization.