Downloaded 48 times


































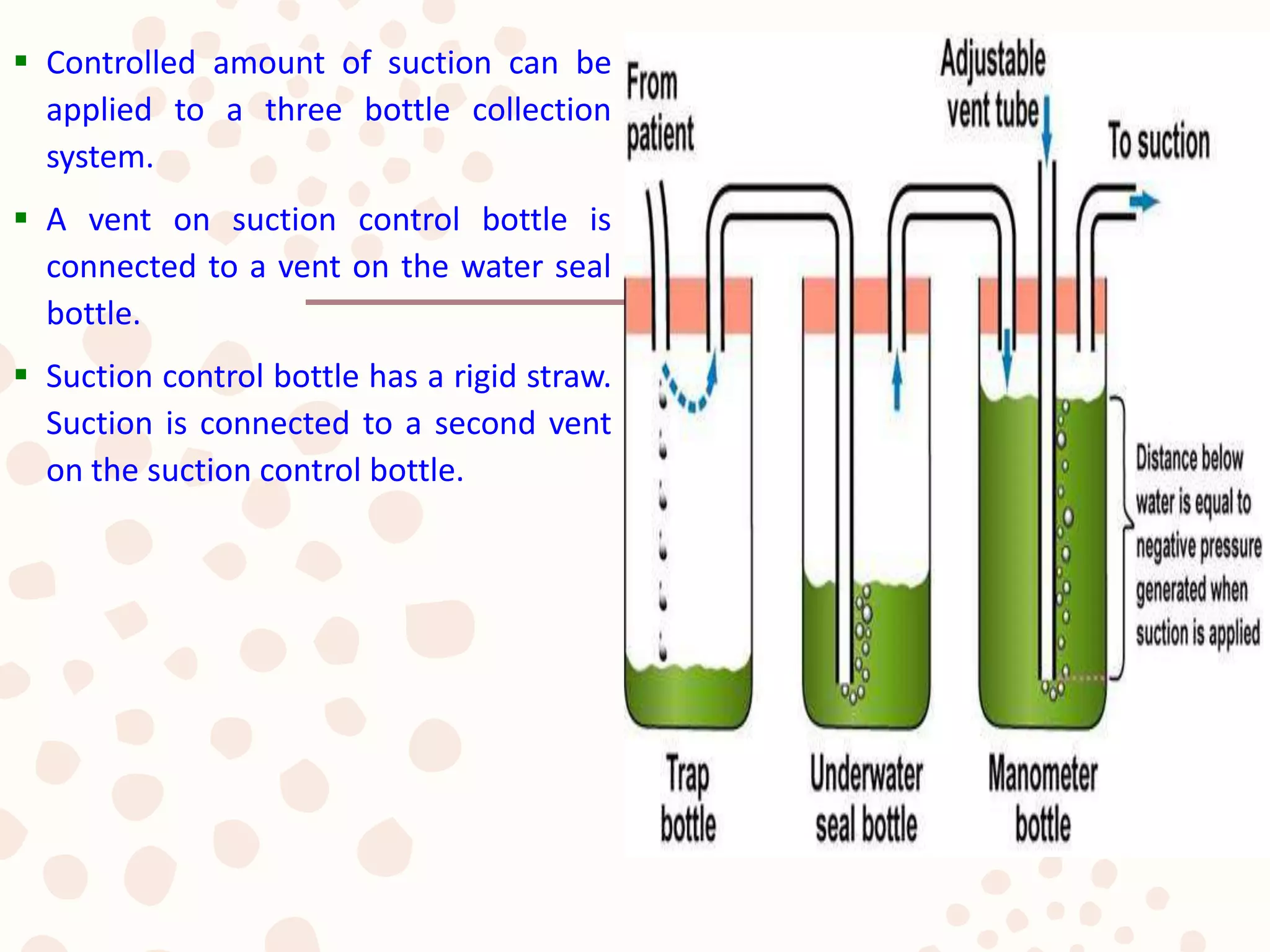





























This document discusses the placement and management of chest drains. It covers indications for chest drains, sites of insertion, types of drainage systems, securing the drain, and troubleshooting potential issues. The key points addressed are how to choose an appropriate chest drain size, ensuring the drain is placed in the correct anatomical location, and using drainage systems that provide controlled suction when needed to drain fluid or air from the pleural space. Complications like an air leak are discussed and methods to differentiate the cause are presented.



































































