Downloaded 1,381 times

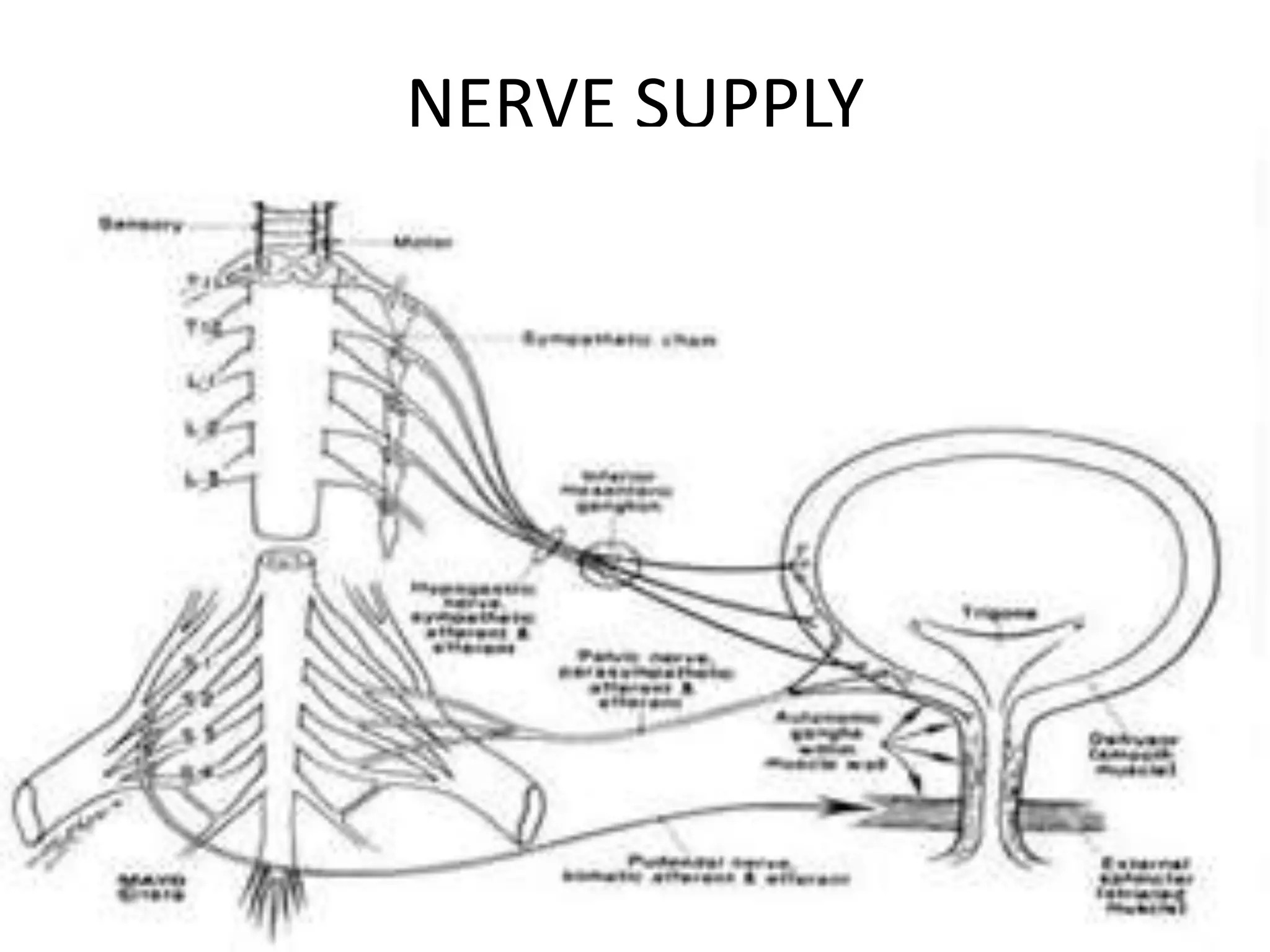


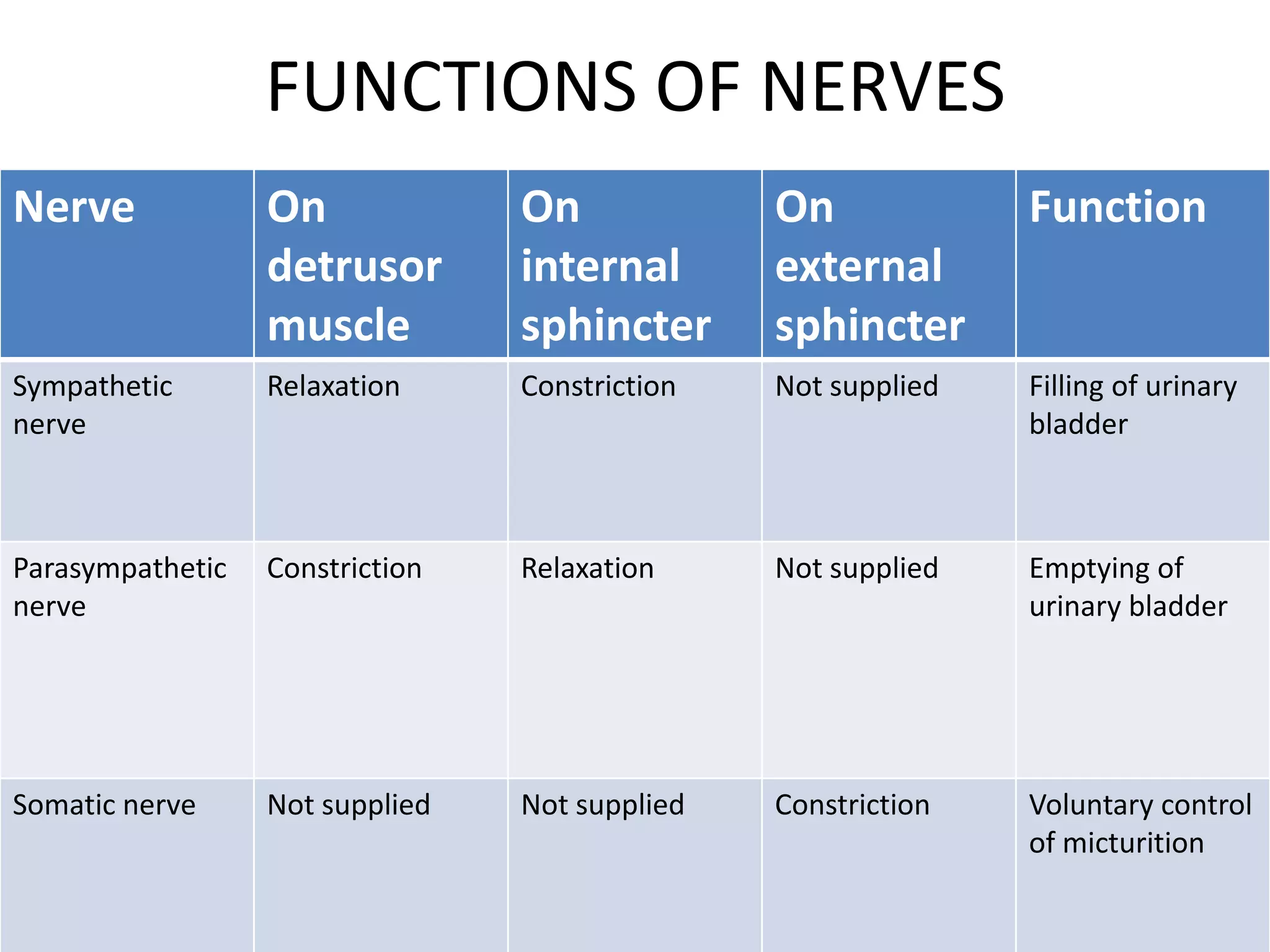
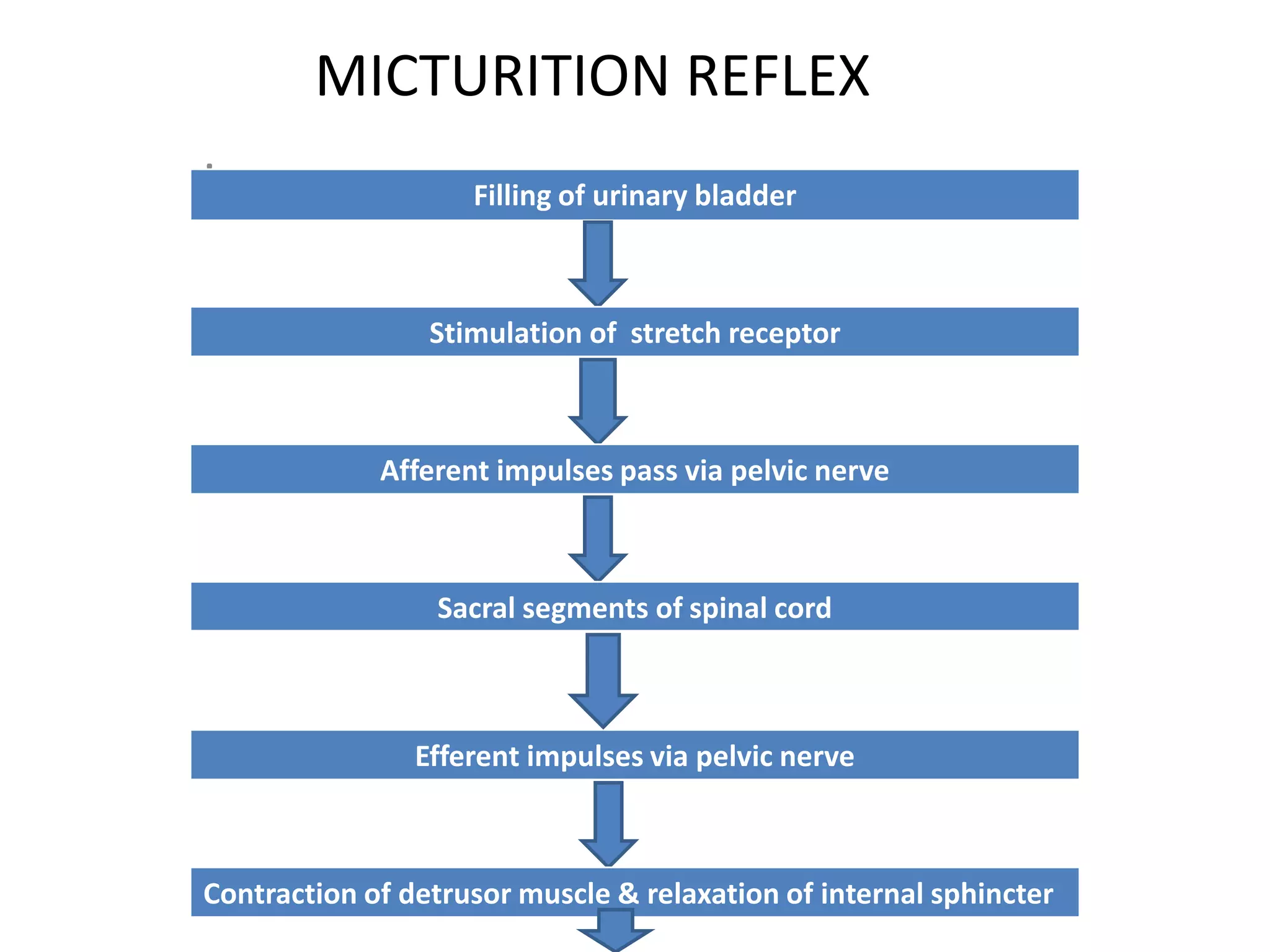

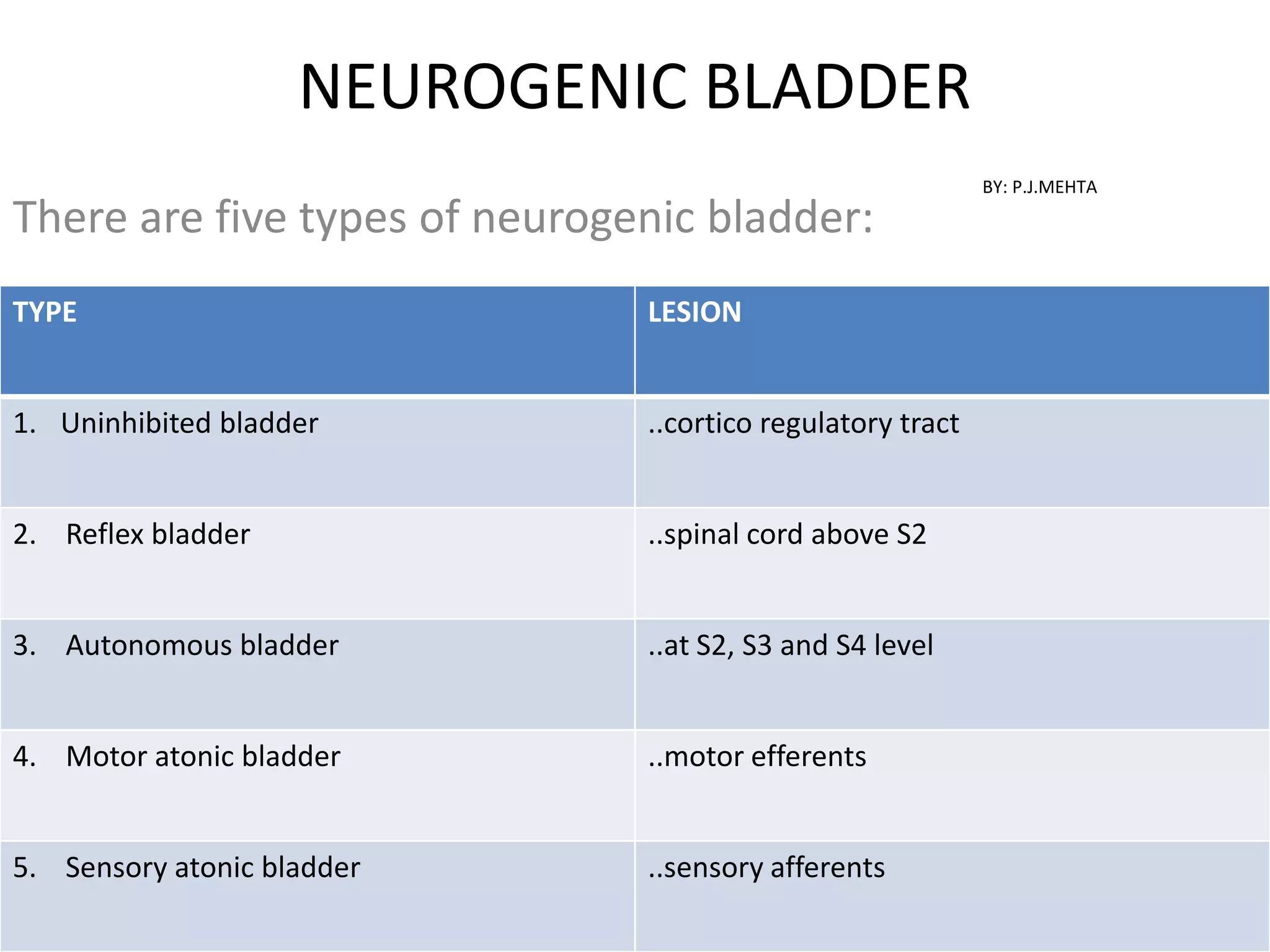

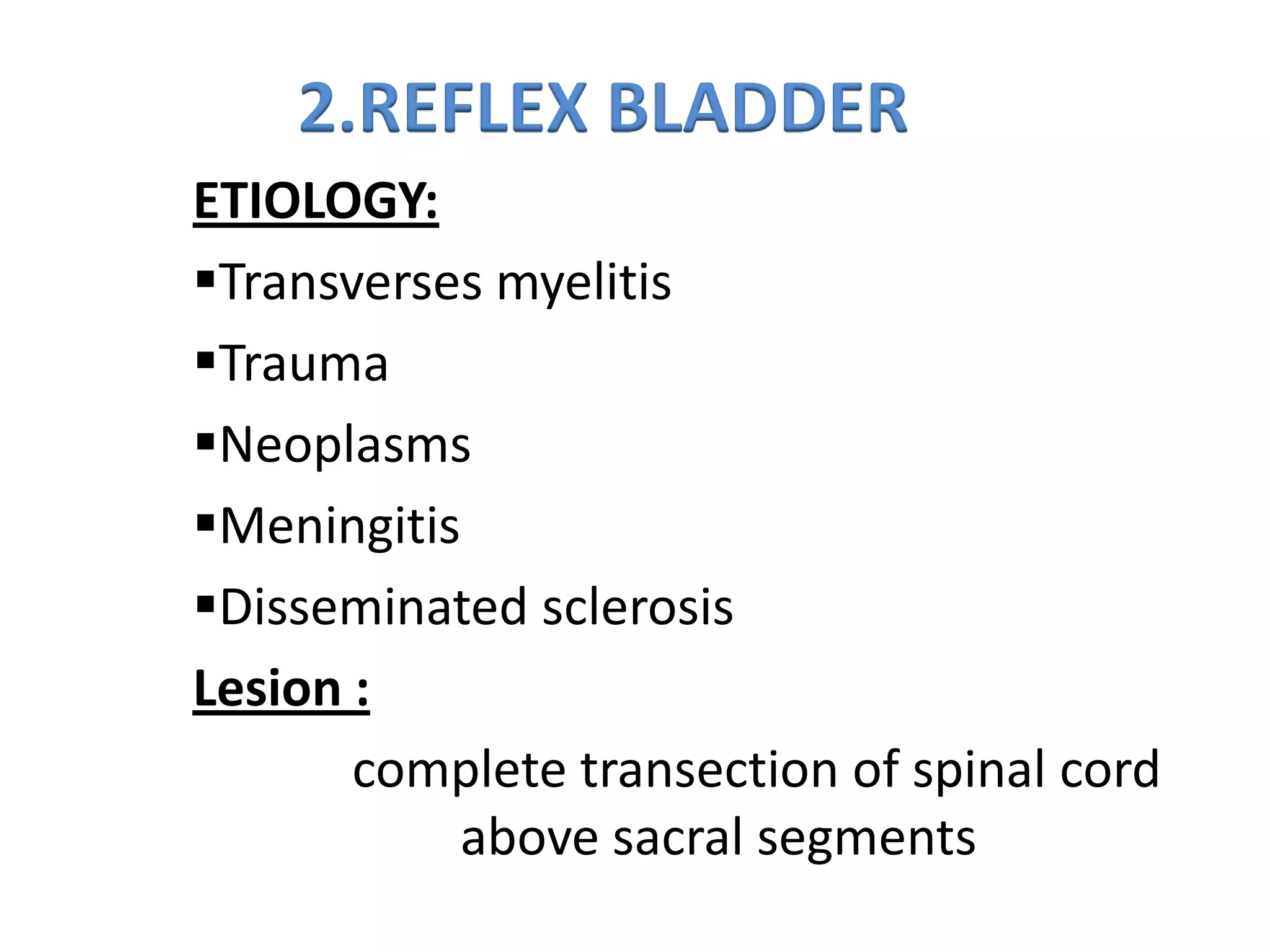


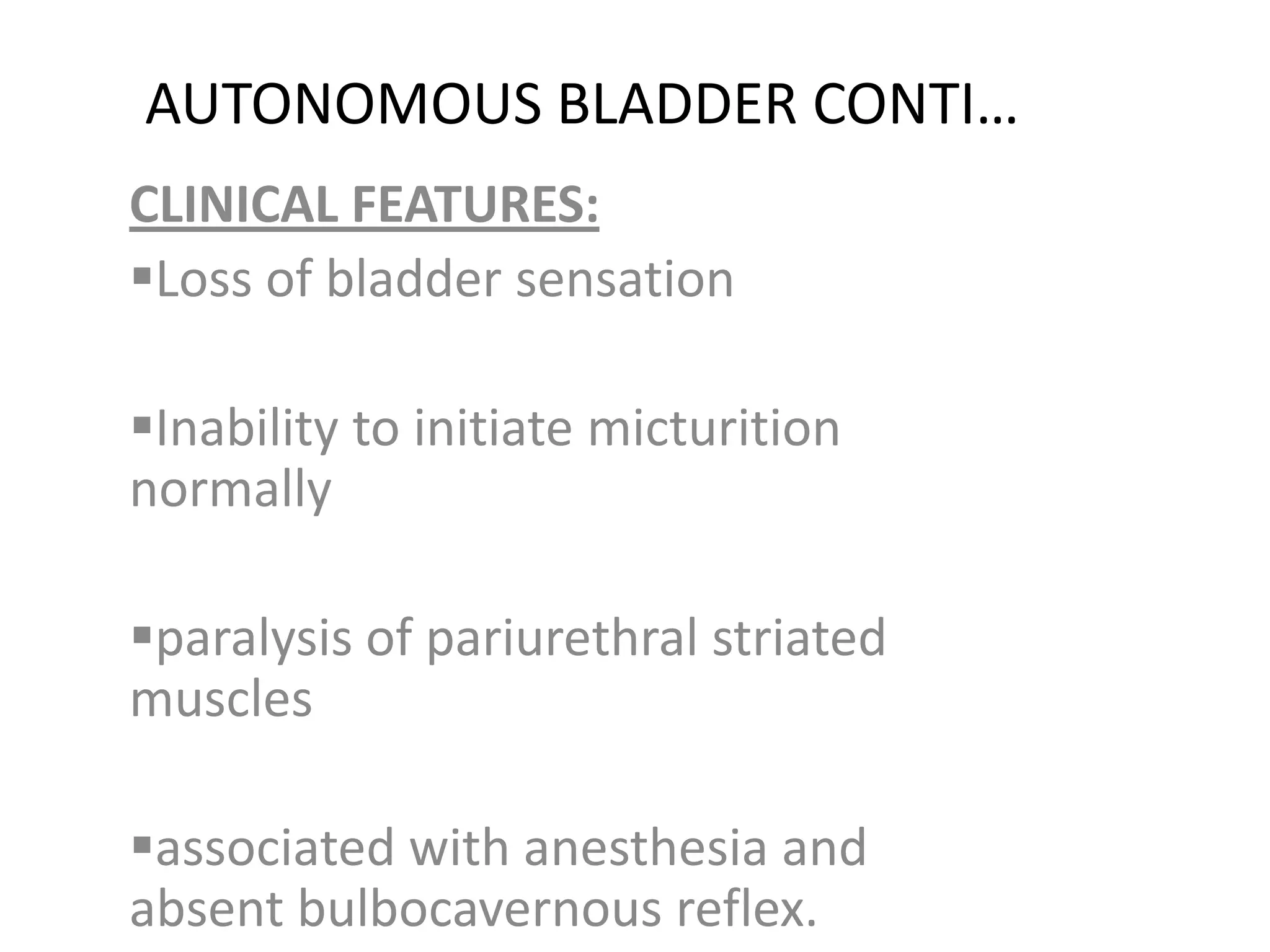











This document discusses the anatomy and physiology of the urinary bladder. It covers the bladder's structure, capacity, nerve supply, micturition reflex, types of neurogenic bladder, and different types of urinary incontinence. The bladder acts as a temporary storage site for urine before it is emptied through the urethra. Its nerve supply and reflex pathways allow for coordinated filling and emptying. Damage to different parts of this system can result in neurogenic bladder disorders or incontinence. The document provides details on each topic.