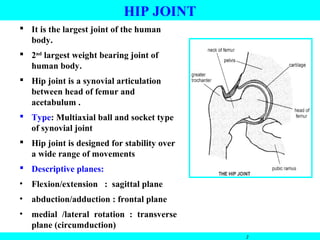
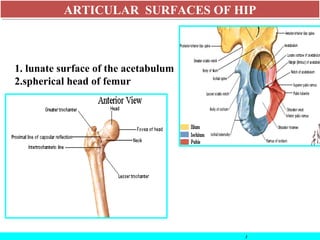
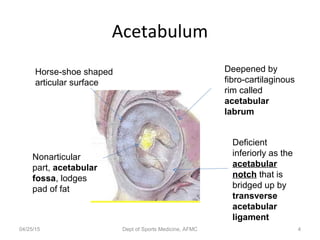
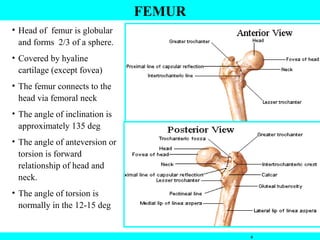
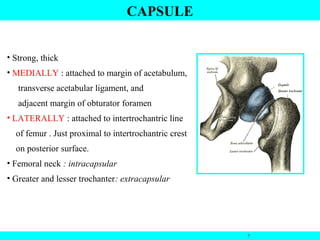
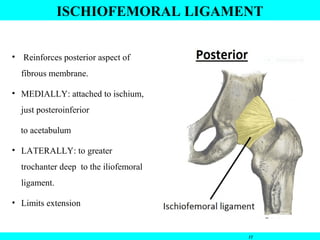
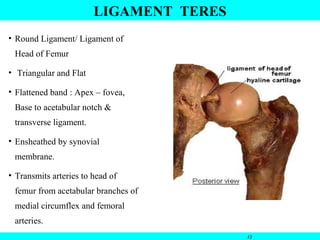
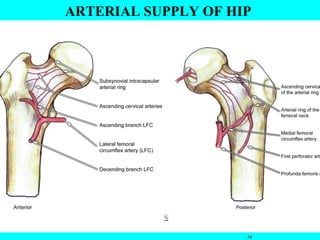
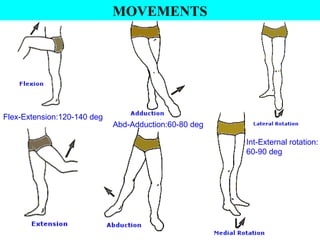
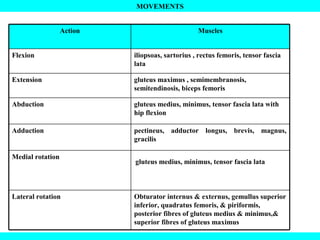
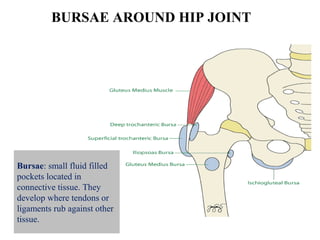
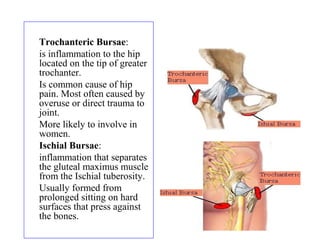
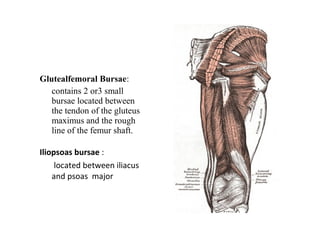
The document summarizes the anatomy and examination of the hip joint. It describes the hip joint as a ball and socket synovial joint between the femoral head and acetabulum. It details the articular surfaces, ligaments, muscles, nerve supply, blood supply and movements of the hip joint. It also discusses the ossification of the hip bone and bursae that can form around the hip joint.