Downloaded 123 times


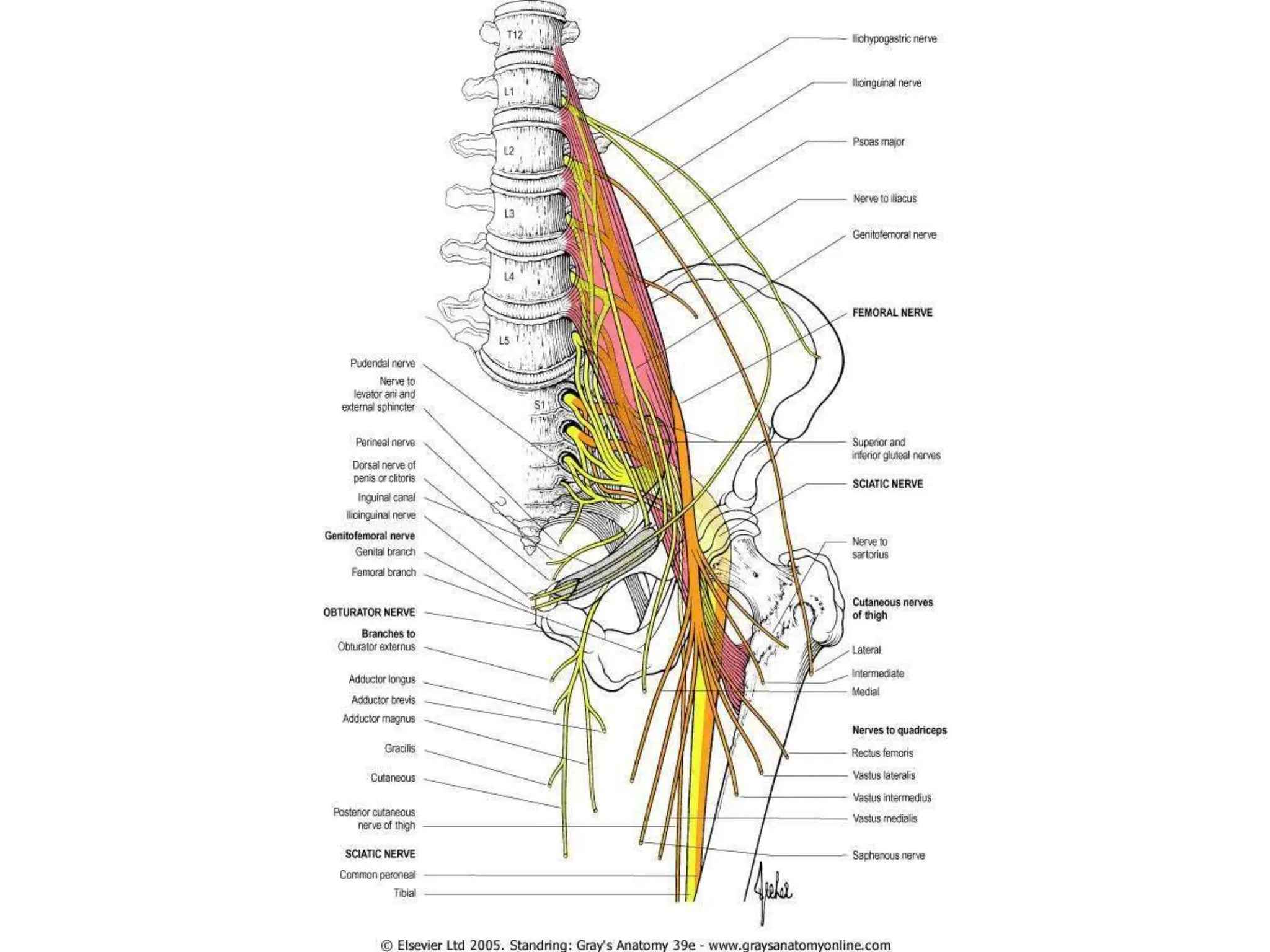
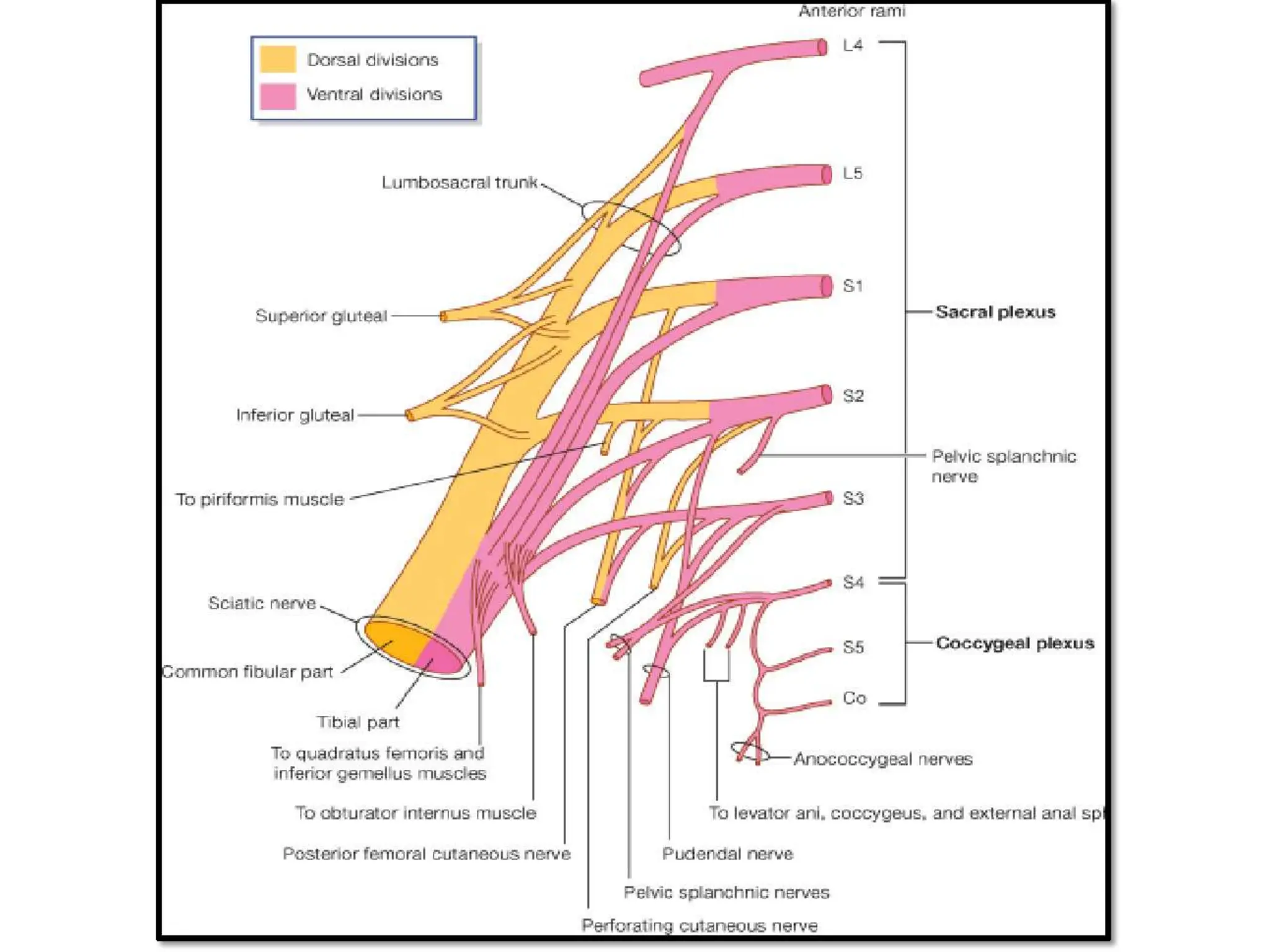

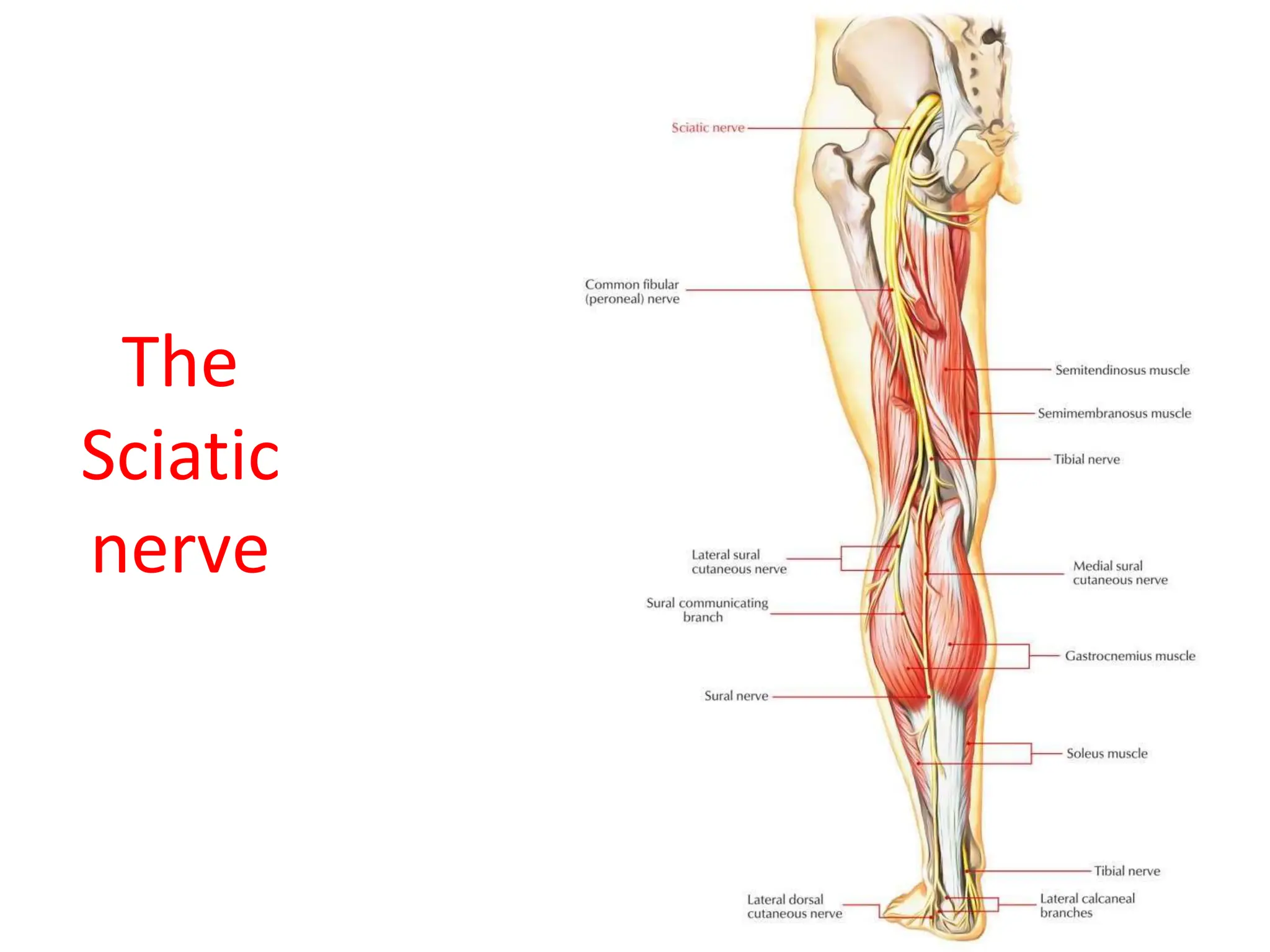
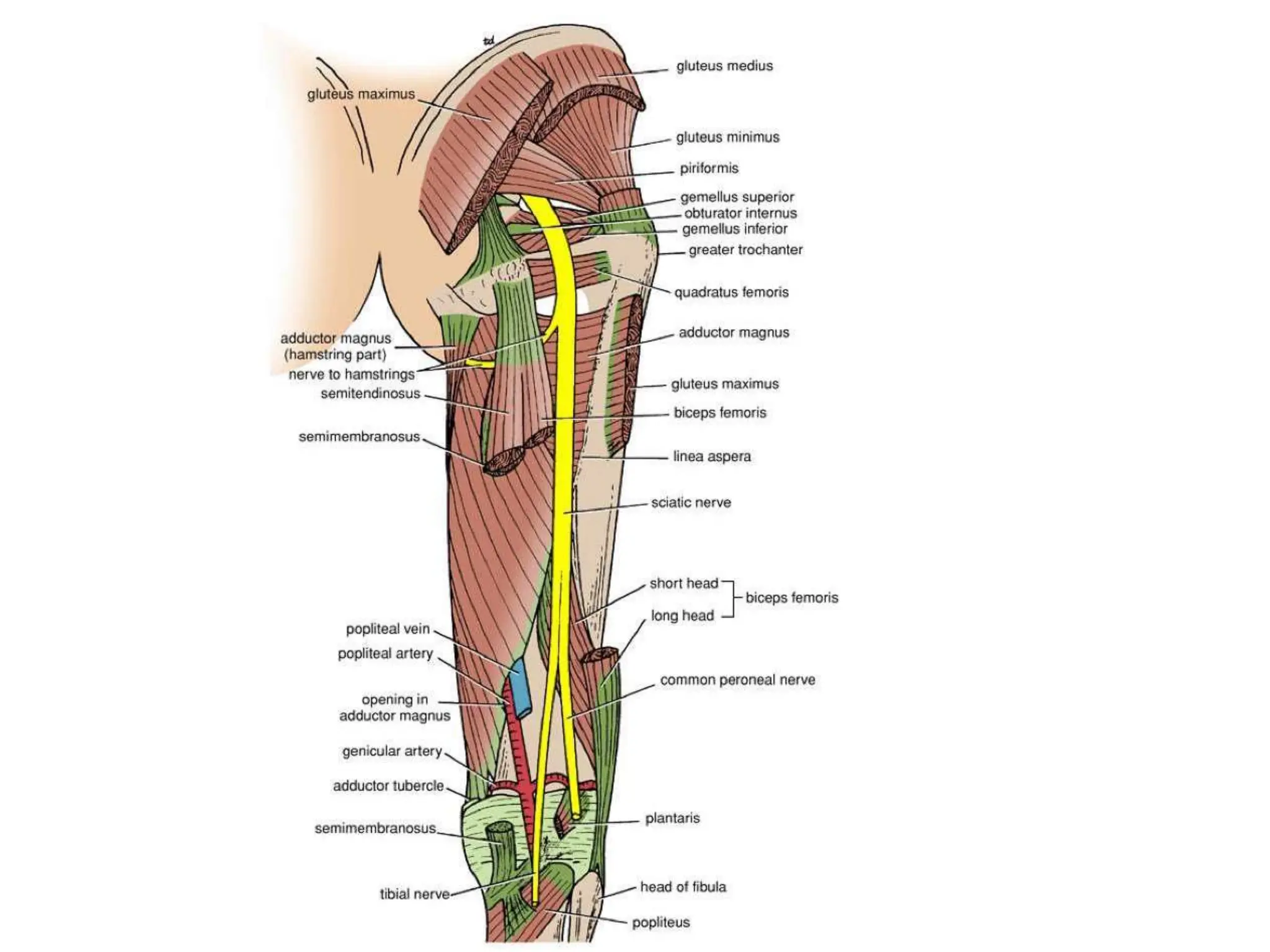

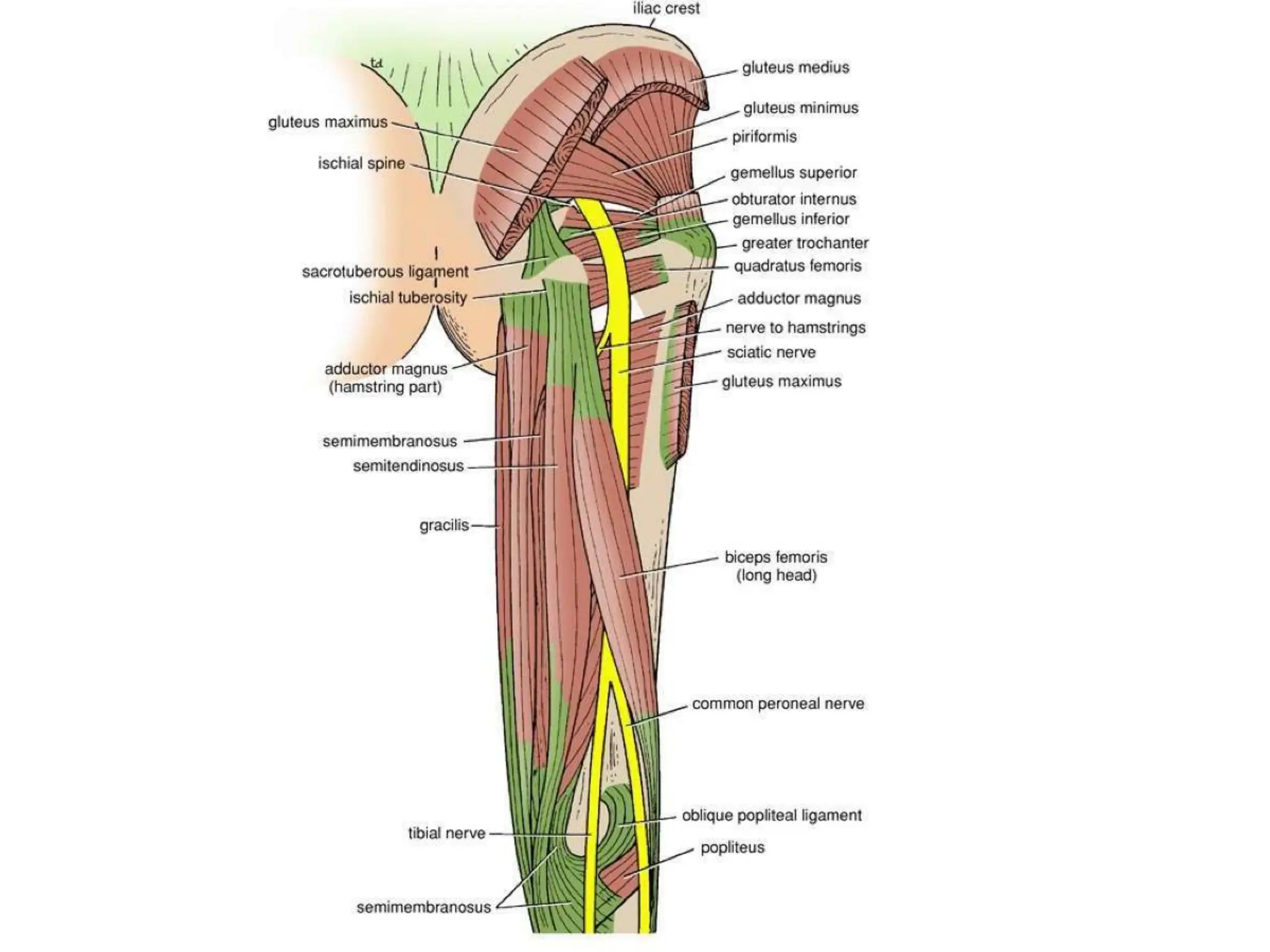

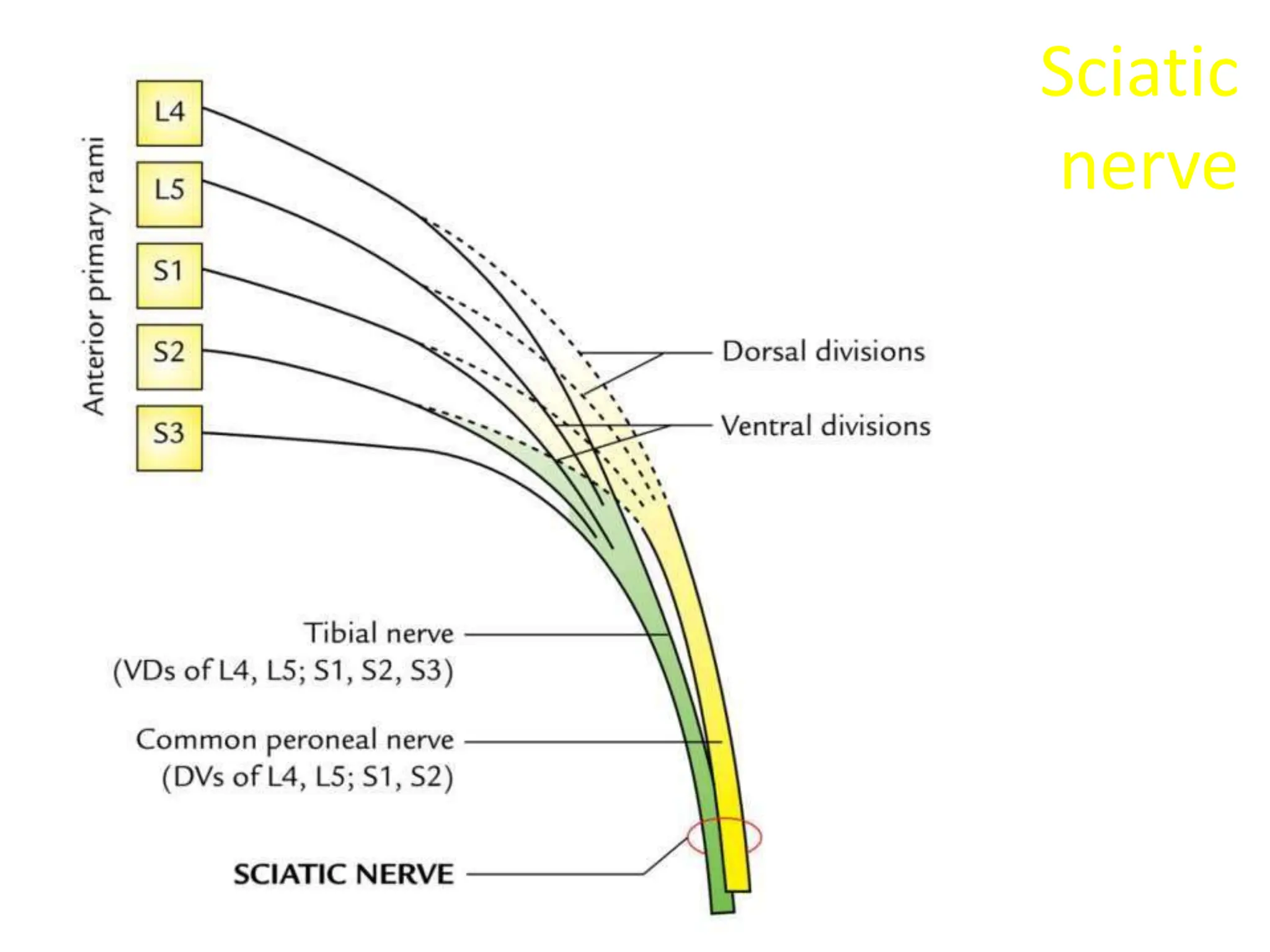
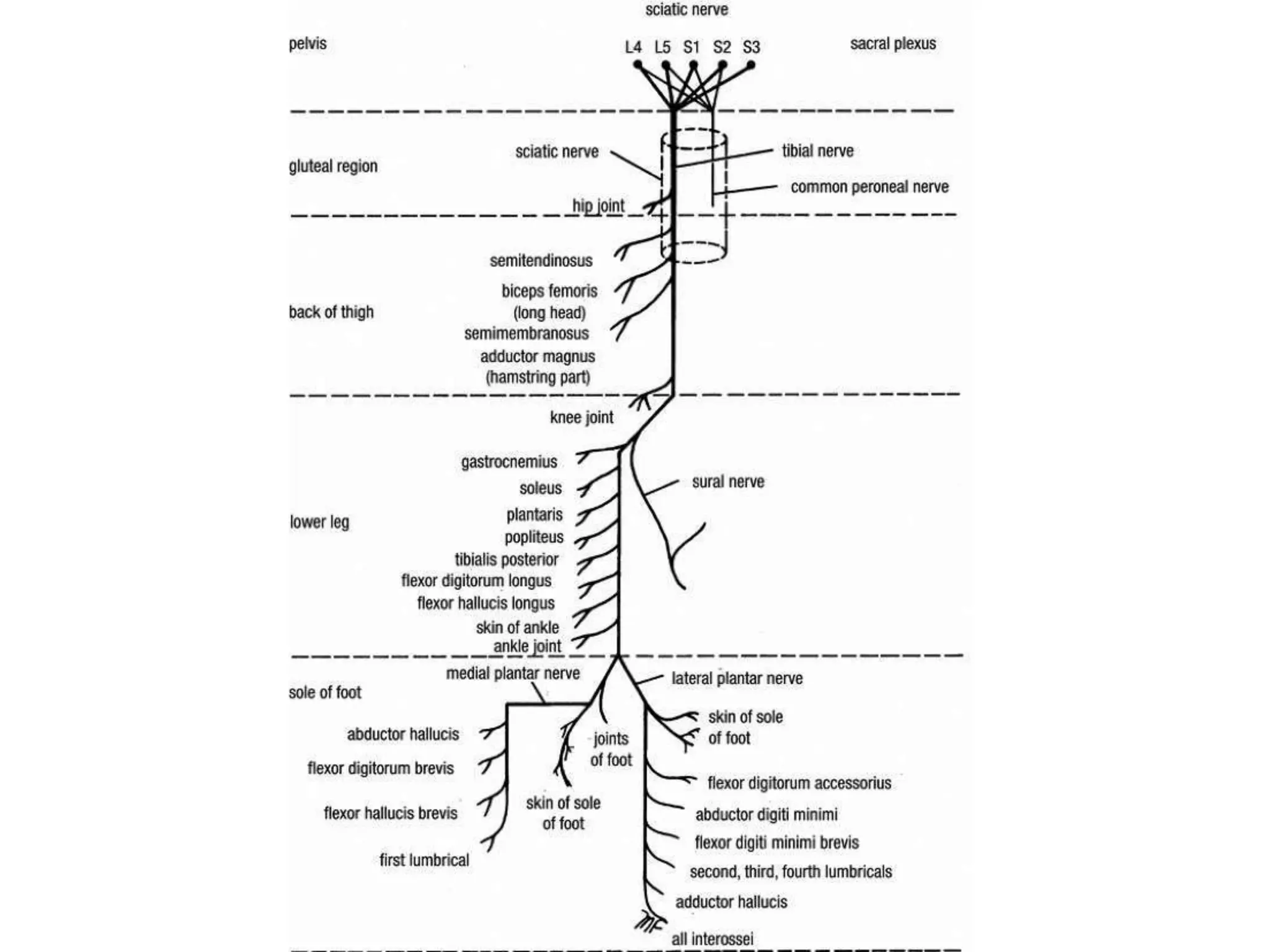
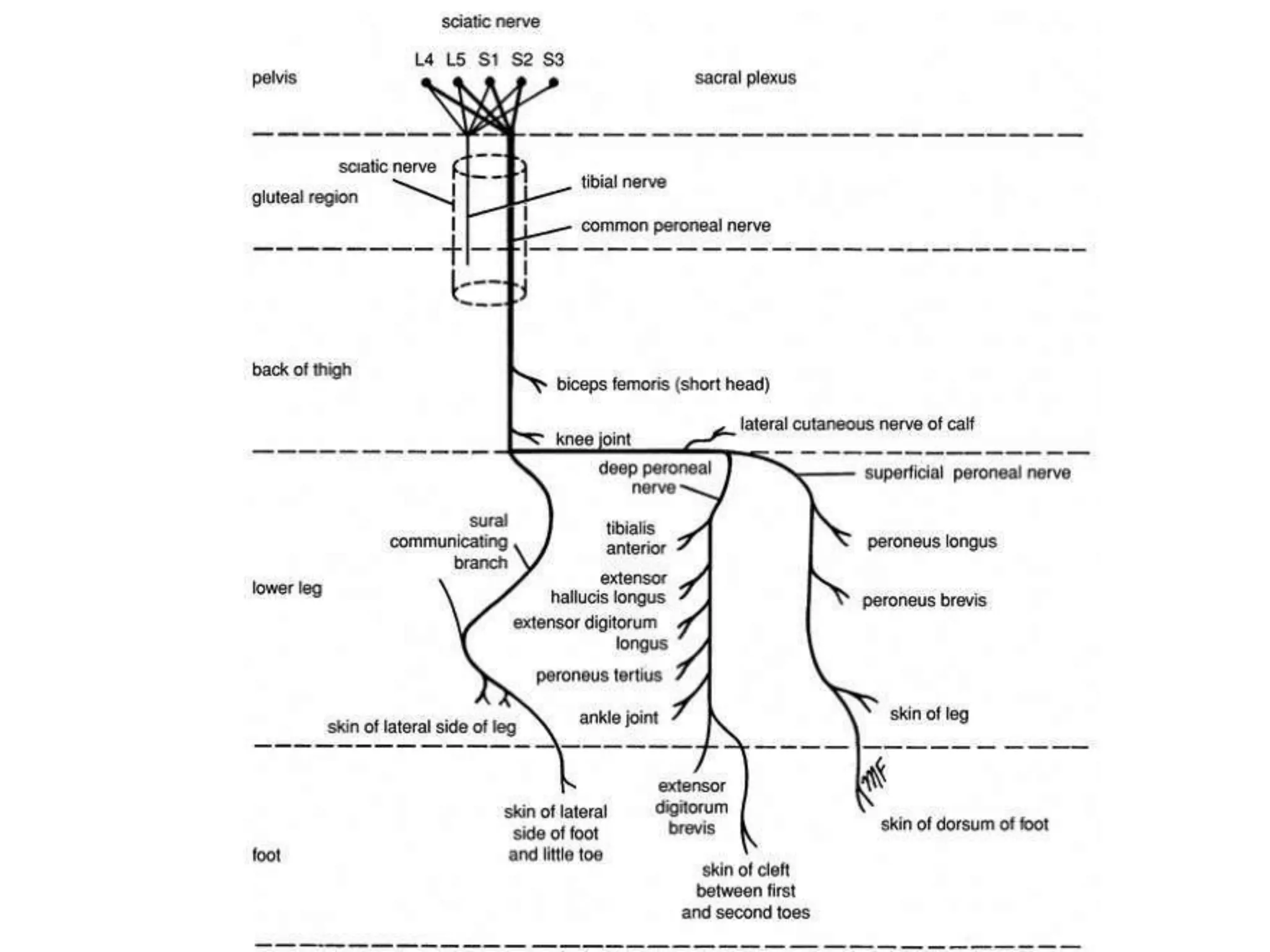



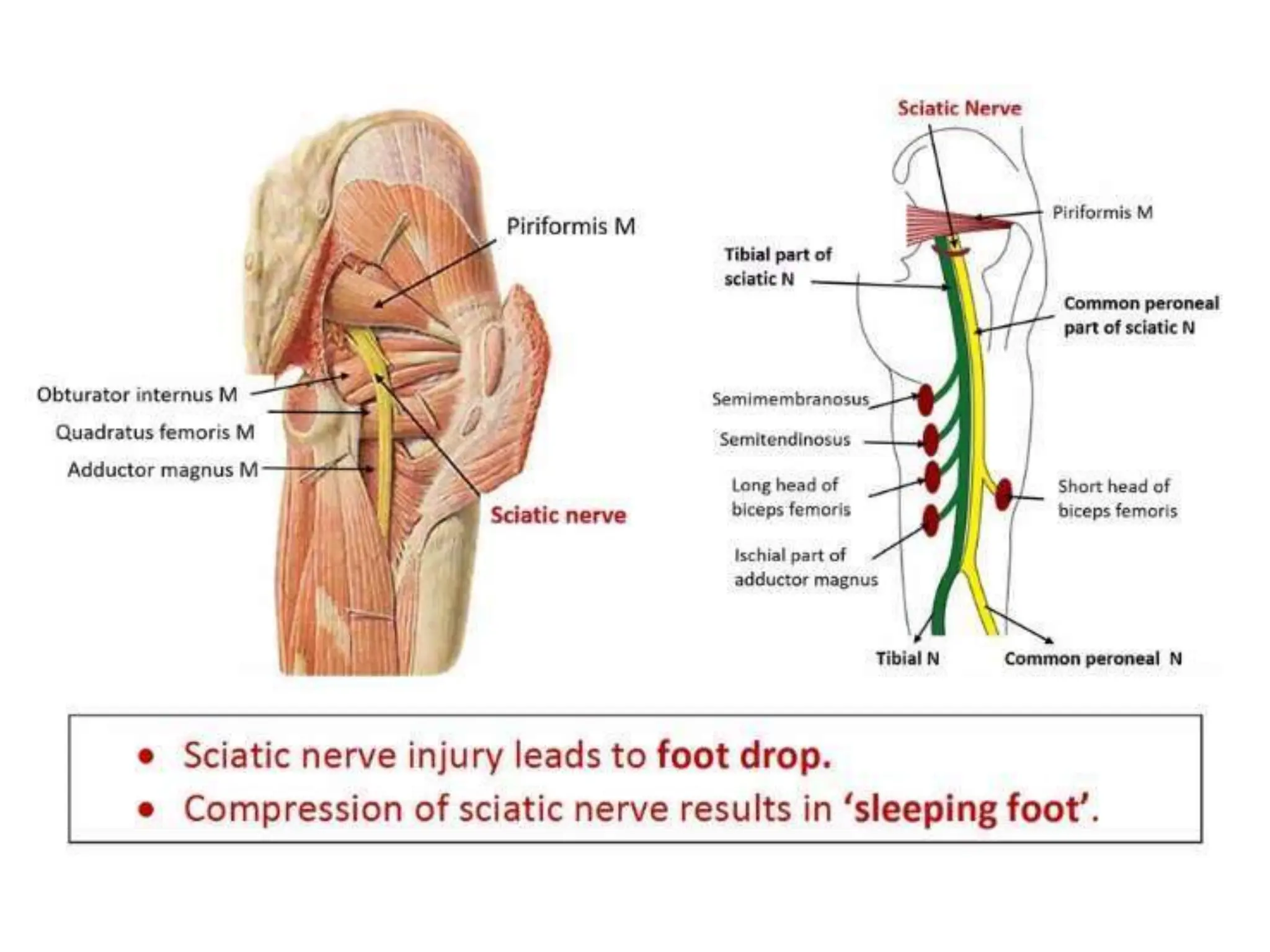
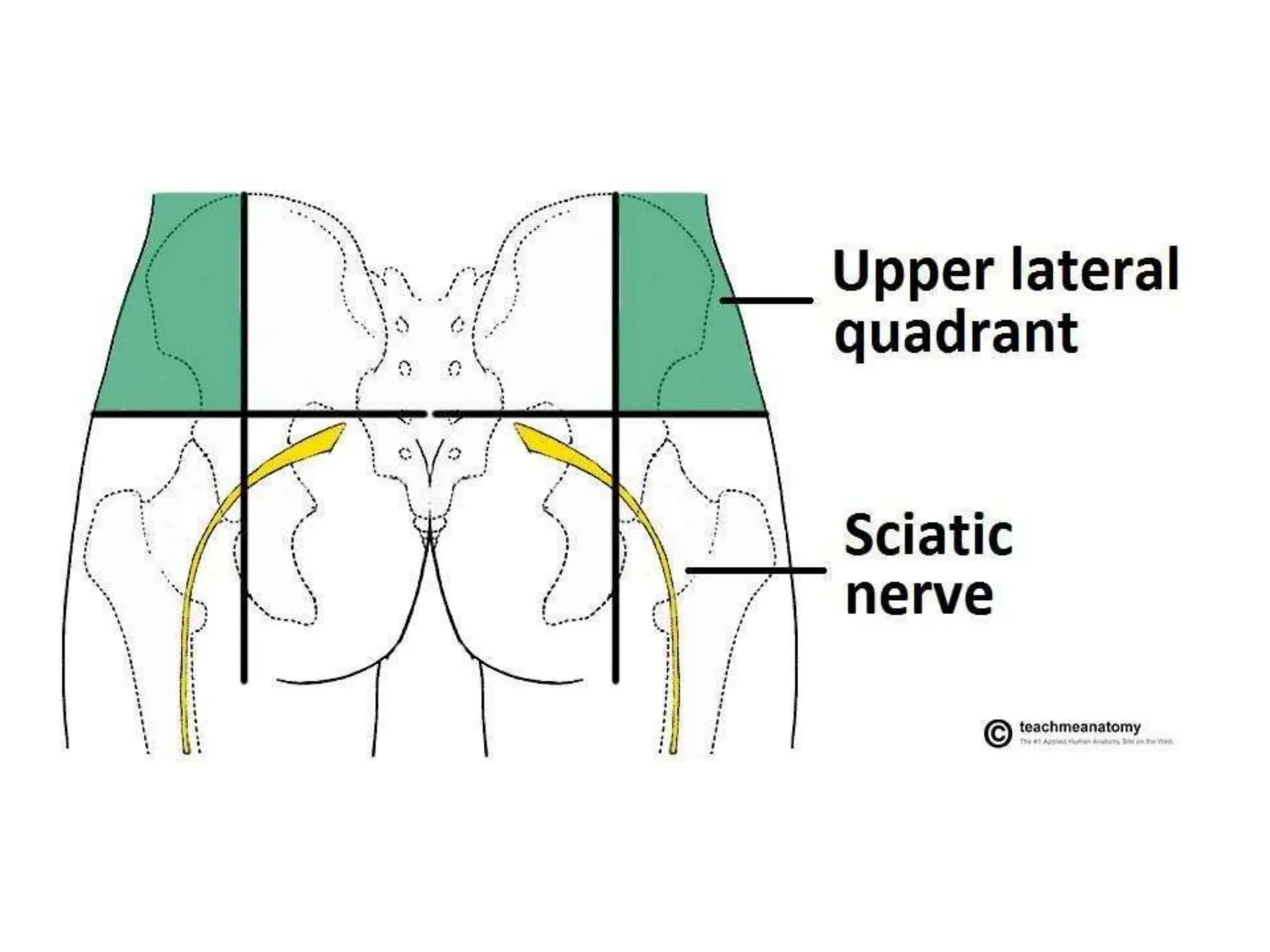
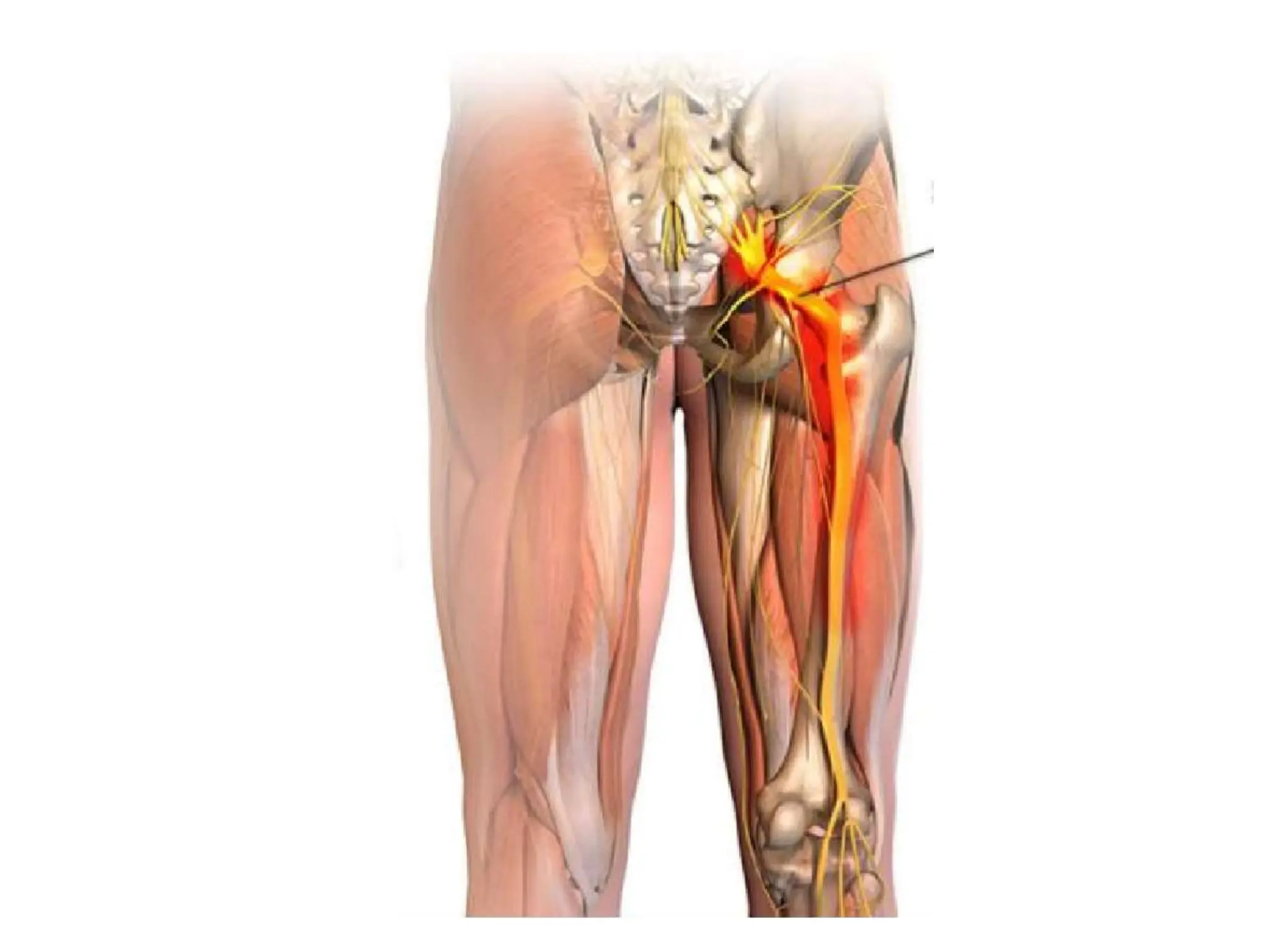








The document details the anatomy of the sciatic nerve, including its origin, course, branches, and clinical significance related to injuries and conditions like sciatica. Key points include the structure being the largest nerve in the body, its role in motor and sensory innervation of the lower limb, and considerations for preventing injury during intramuscular injections. Additionally, it outlines specific case studies of sciatic nerve injury and their manifestations.























































































