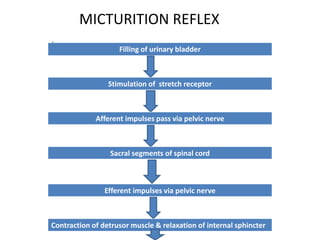
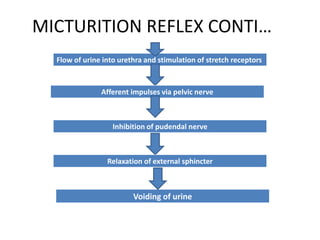
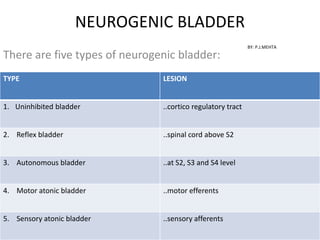
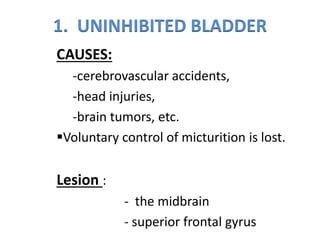
The document provides a comprehensive overview of neurogenic bladder, including its anatomy, nerve supply, and various types of neurogenic bladder dysfunctions. It covers the physiological mechanisms, common causes of different bladder types, and the management of urinary incontinence and retention. Additionally, it outlines treatment options like catheterization, drug therapy, and surgical interventions for affected individuals.