
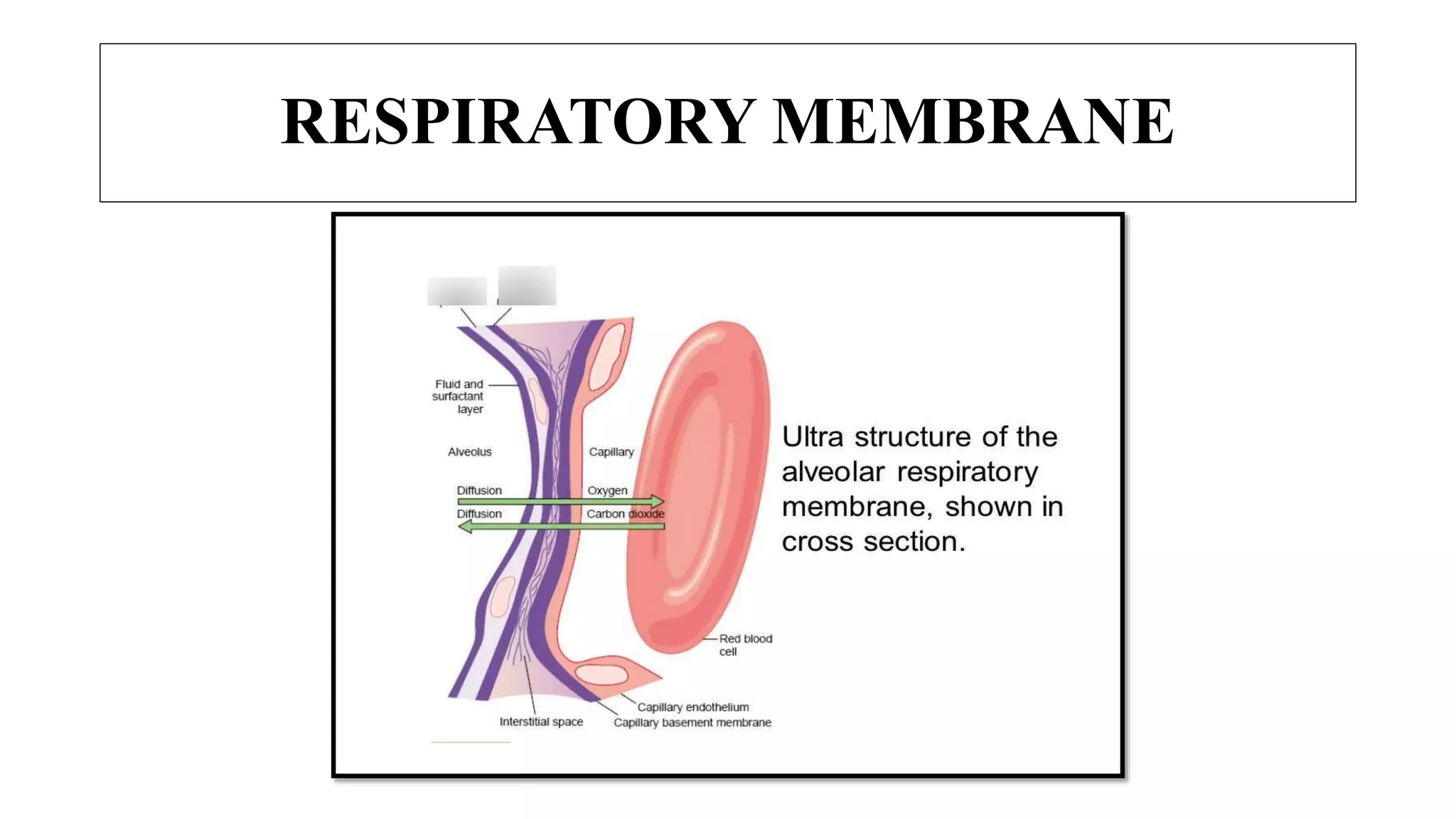
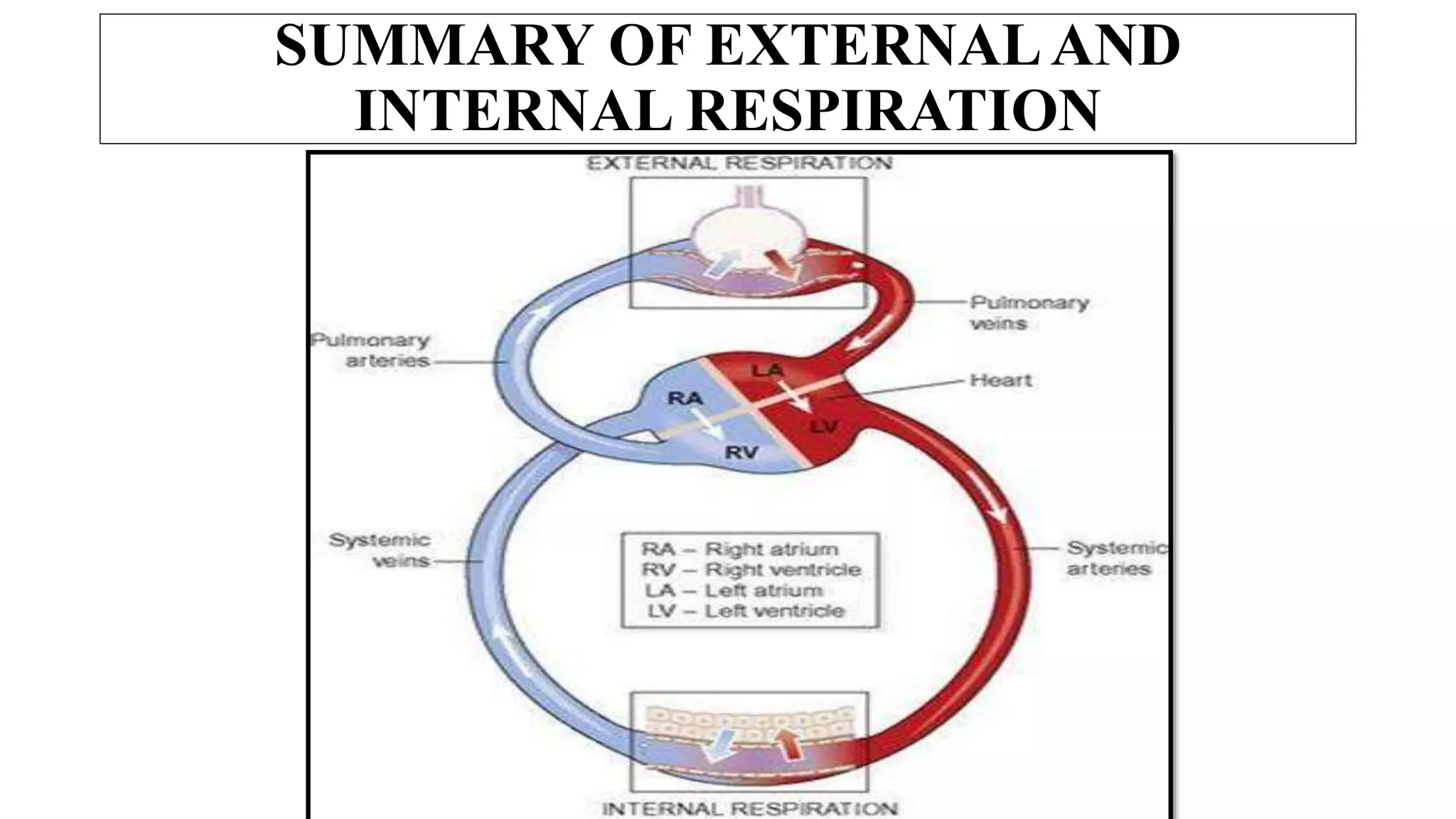
![Exchange of gases between the blood and the lungs is called external
respiration.
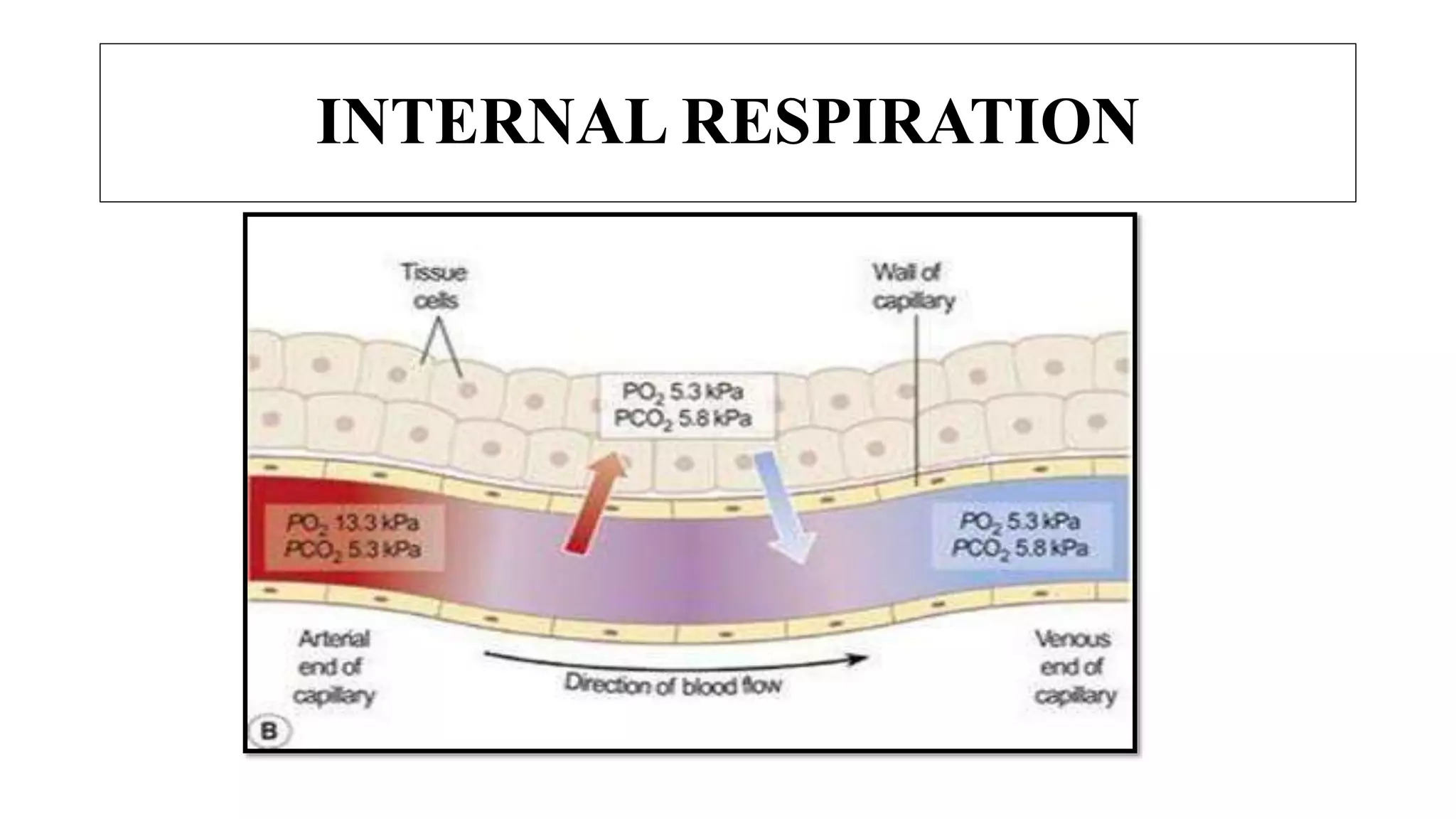
Exchange of gases between the blood and the cells is called internal
respiration.
The organs of respiratory system are:
INTRODUCTION
• Nose - Bronchioles & smaller air passages
• Pharynx - Two lungs and their covering, pleura
• Larynx - Muscles of breathing : [intercostal
• Trachea - muscles and Diaphragm]
• Two bronchi (one in each lung)](https://image.slidesharecdn.com/therespiratorysystem-210806052614/75/The-respiratory-system-3-2048.jpg)





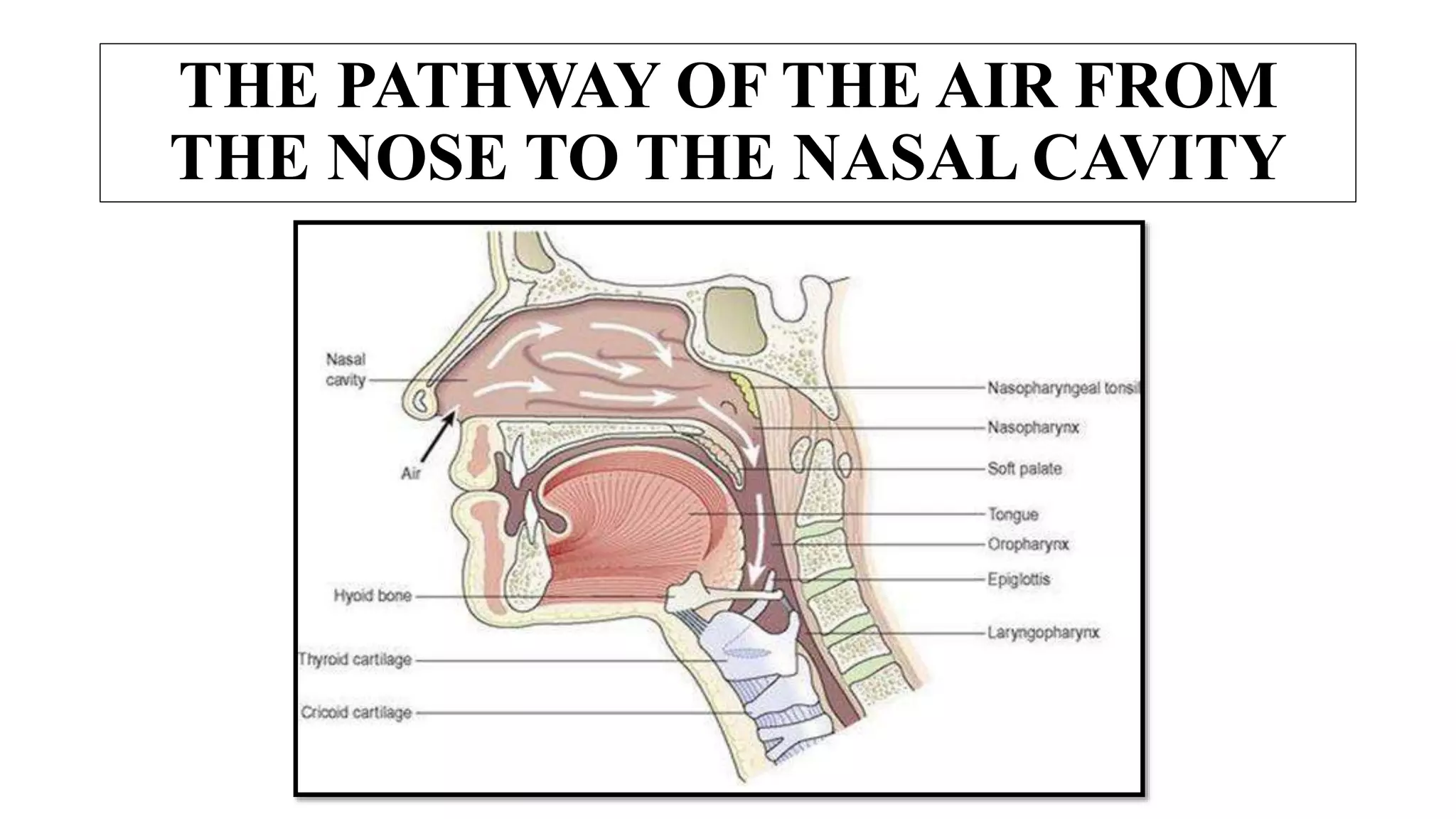




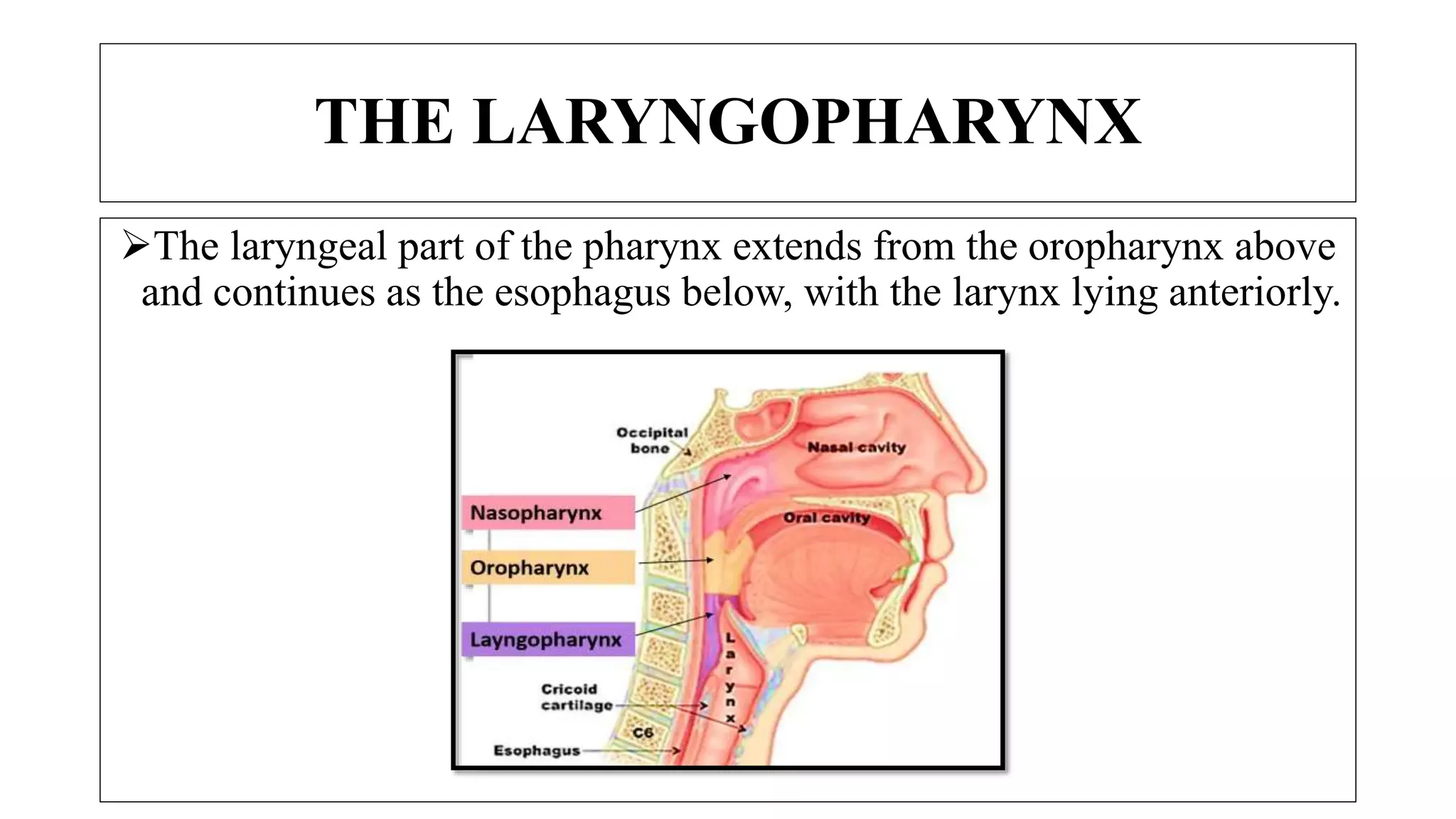





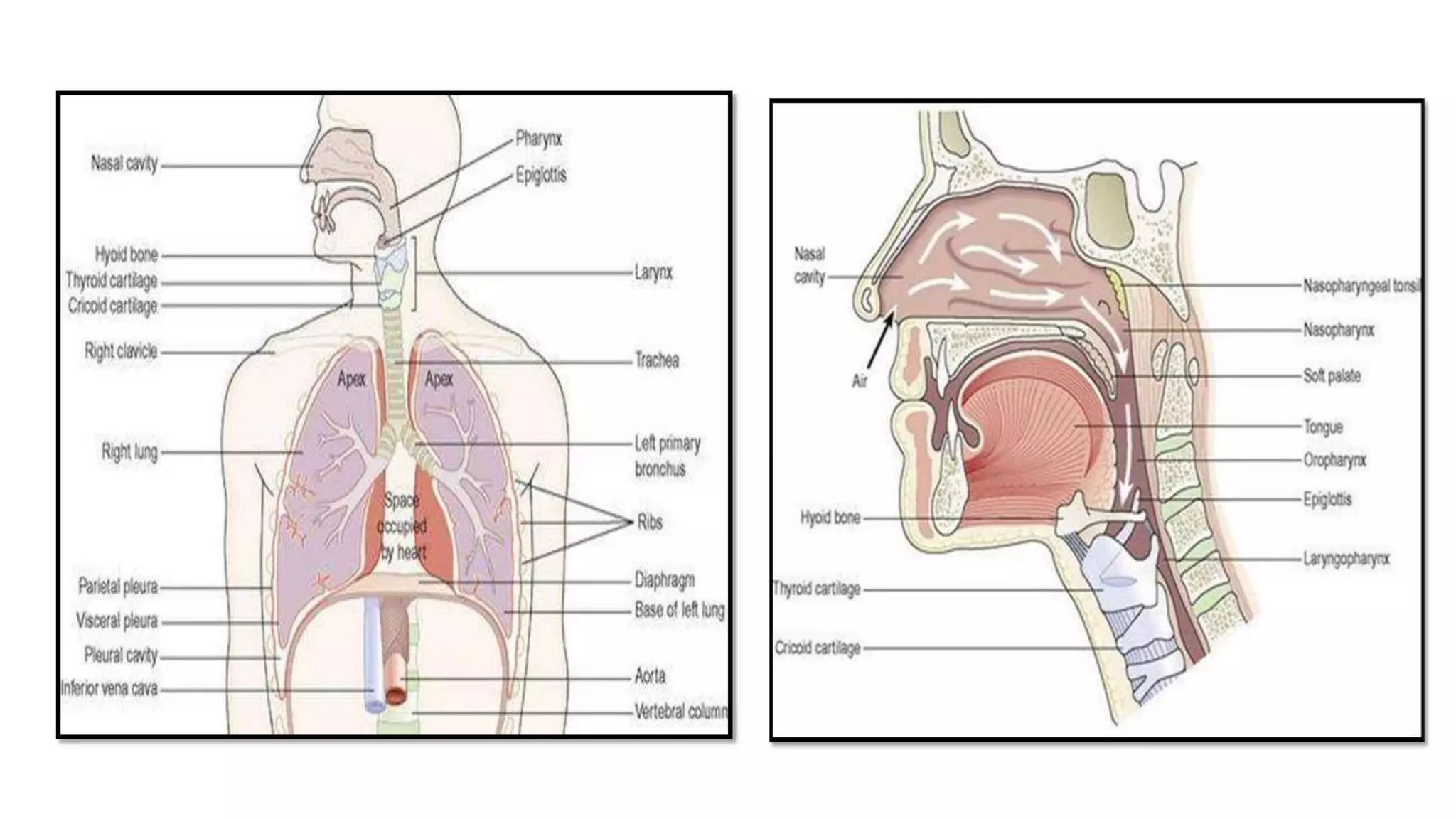

























































The respiratory system provides oxygen to the body's cells and removes carbon dioxide. It includes the nose, pharynx, larynx, trachea, bronchi and lungs. The nose warms, filters and humidifies inhaled air and is also the organ of smell. The pharynx is a passageway for air and food that is lined with lymphoid tissue including the tonsils. The larynx, or voice box, contains cartilages including the thyroid and cricoid cartilages which support the vocal cords that produce sound.








































![The respiratory system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/therespiratorysystemautosaved-221121115106-26ae7a7b-thumbnail.jpg?width=640&height=640&fit=bounds)














































