Downloaded 259 times

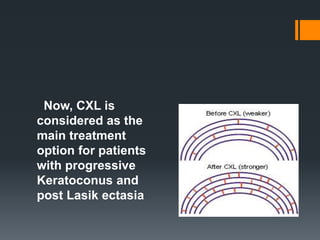




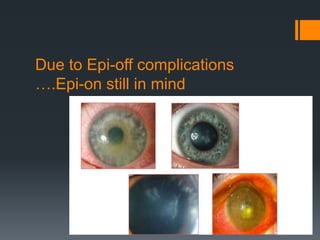
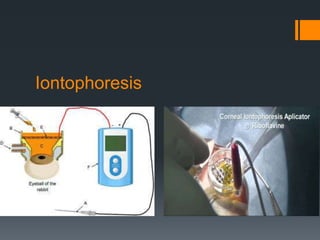






The document discusses recent advancements in corneal collagen cross-linking (CXL) techniques aimed at treating progressive keratoconus and post-LASIK ectasia. It highlights the comparison between epithelium-on and epithelium-off CXL, as well as the efficacy of iontophoresis and modified protocols for thin corneas. Additionally, it emphasizes the need for aggressive treatment strategies in pediatric patients with keratoconus and the importance of further research for various CXL techniques, especially in cases of infectious keratitis.




































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




