• Photo-polymerization usingUV-light was found to be the
most promising technique to achieve cross-links in
connective tissue.
• Photo-polymerization is activated by means of a non-
toxic and soluble photomediator and a wavelength which
is absorbed strongly enough to protect deeper layers of
the eye (riboflavin-UVA technique).
• UV-A radiation with concomitant administration of
riboflavin/dextran solution as a photosensitizer generates
singlet oxygen and superoxide free radicals. This
process leads to physical cross-linking of the corneal
collagen fibers.
4.
• Intrahelical orinterhelical cross-links can be
formed within or between the tropocollagen units
that comprise the individual collagen fibrils; and,
intermicrofibrillar cross-links can form between
adjacent collagen microfibrils that comprise the
collagen lamellae.
• Thus, progressive corneal thinning is slowed
down or even stopped. Biomechanical
strength of corneal tissue is improved by a
factor of up to 4
5.
Purpose of procedure
•increase the cornea's mechanical stability
• to stop progression of bulging and thinning
of the cornea
• to prevent the need for corneal
transplantation
6.
indications
• treat alldiseases that require
biomechanical stabilization of the cornea
– Keratoconus
– corneal melting
– iatrogenic keratectasia after refractive lamellar
surgery
– pellucid marginal degeneration
– Also in combination with other surgical
procedures, such as intracorneal rings
Preoperative evaluation
• preoperativeconsultation, the following
examinations are mandatory
– UCVA
– BSCVA
– MRSE
– IOP
– Pachymetry
– topography and difference maps
– K values
– ECC
9.
Procedure
• proparacaine 0.5%for up to thirty minutes
before UVA exposure (approximately two drops
every five minutes).
• the riboflavin is then applied onto the cornea for
up to 25 minutes before irradiation
• 30-minute exposure to UVA light (370 nm
fluence at 3mW/cm2 ) to the central 8 mm of the
cornea with speculums in place
• The riboflavin solution must be reapplied to the
cornea every three minutes during the UVA
irradiation.
10.
• After removalof the corneal epithelium
riboflavin/dextran solution is instilled for 30
minutes (1 drop every 2 minutes).
• Then the corneal penetration of is checked
under a slit lamp by establishing that
the anterior chamber is slightly yellow.
• Pachymetry is performed to make sure
that minimum corneal thickness is
maintained.
11.
• UV-A irradiationstarts using the device under
continued administration of riboflavin/dextran
solution 1 drop every 2 minutes.
• After 30 minutes of radiation the treatment is
finished
• the patient receives post-op treatment like after
PRK:
– bandage contact lens
– Painkiller
– Steroids
– Antibiotics
– artificial tears.
12.
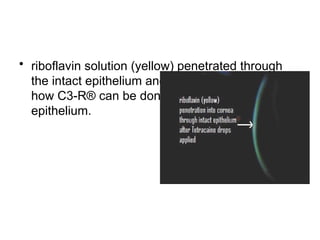
• riboflavin solution(yellow) penetrated through
the intact epithelium and into the cornea which is
how C3-R® can be done without scraping off the
epithelium.
13.
• it mustbe explained to the patient that an
improvement in visual acuity must be
considered as a bonus rather than a goal.
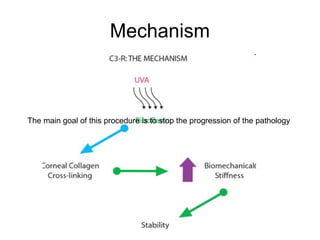
• The main goal of this procedure is to stop
the progression of the pathology
14.
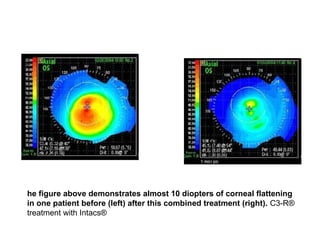
he figure abovedemonstrates almost 10 diopters of corneal flattening
in one patient before (left) after this combined treatment (right). C3-R®
treatment with Intacs®
15.
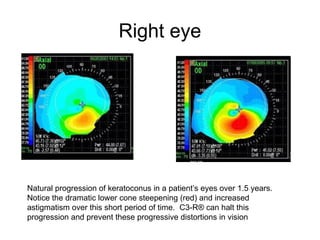
Right eye
Natural progressionof keratoconus in a patient’s eyes over 1.5 years.
Notice the dramatic lower cone steepening (red) and increased
astigmatism over this short period of time. C3-R® can halt this
progression and prevent these progressive distortions in vision
16.
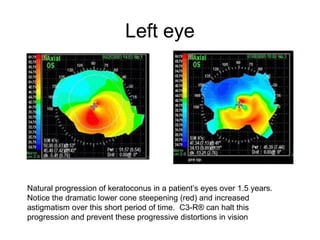
Left eye
Natural progressionof keratoconus in a patient’s eyes over 1.5 years.
Notice the dramatic lower cone steepening (red) and increased
astigmatism over this short period of time. C3-R® can halt this
progression and prevent these progressive distortions in vision
17.
• a significantincrease in BCVA in more than 85%
of the treated eyes.
• Six months after corneal cross linking, the
refractive cylinder is reduced in over 80% of the
eyes.
• Consequently corneal cross linking induces
a restoring biomechanical force upon the
deformed corneal shape.
• The steepest K-value is usually decreased by 1
Diopter and the percentage of eyes that had a
clinical relevant reduction exceeds 86%.
18.
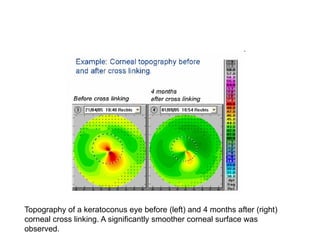
Topography of akeratoconus eye before (left) and 4 months after (right)
corneal cross linking. A significantly smoother corneal surface was
observed.
19.
• An increaseof one to two lines was
observed between 9 to 30 months after
the treatment.
• Increases of up to three or four lines
were observed from 30 to 60 months.
20.
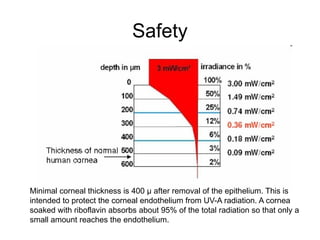
Safety
Minimal corneal thicknessis 400 µ after removal of the epithelium. This is
intended to protect the corneal endothelium from UV-A radiation. A cornea
soaked with riboflavin absorbs about 95% of the total radiation so that only a
small amount reaches the endothelium.
21.
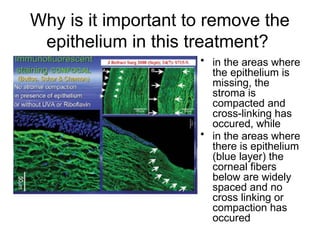
Why is itimportant to remove the
epithelium in this treatment?
• in the areas where
the epithelium is
missing, the
stroma is
compacted and
cross-linking has
occured, while
• in the areas where
there is epithelium
(blue layer) the
corneal fibers
below are widely
spaced and no
cross linking or
compaction has
occured
Editor's Notes
#2 riboflavin is applied to the cornea and it penetrates for approximately 200 μm. The irradiation of the riboflavin molecules by UVA causes them to lose their internal chemical balance, producing oxygen free radicals. At this point, the riboflavin molecule is unstable and becomes stable only when it is linked to two collagen fibrils. It creates a crossed bridge between the collagen fibrils (cross-linking), thus producing a general strengthening of the cornea