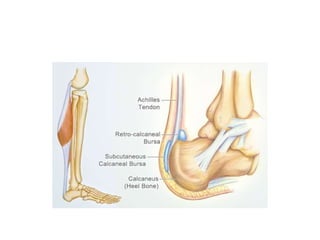
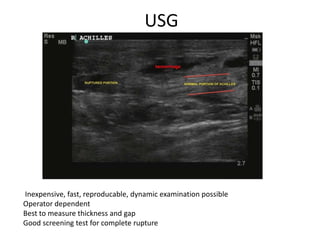
The Achilles tendon connects the calf muscles to the heel bone and is active during walking, running, and jumping. It is vulnerable to rupture, which commonly occurs in the watershed area 2-6cm above the heel in males ages 25-50 during sports. Diagnosis involves physical exam findings like inability to raise the toes and a gap or defect being felt. Treatment options include immobilization in a cast or surgical repair, with the goal of restoring proper tension and length. Post-operative care focuses on protecting the repair during healing over 6 months using casts, braces, and physical therapy.