- Scurvy is a disease caused by vitamin C deficiency that results from a lack of vitamin C in the diet for several weeks. It impairs collagen formation and causes hemorrhaging in tissues.
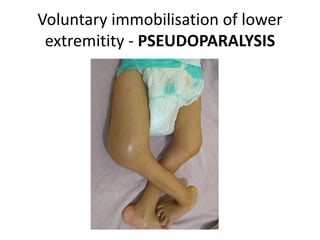
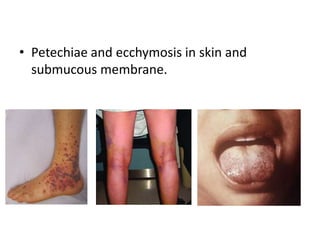
- Symptoms include bleeding gums, loose teeth, bruising of the skin, and bone fractures. In infants, scurvy can cause pseudoparalysis and swelling over bones from subperiosteal hemorrhaging.
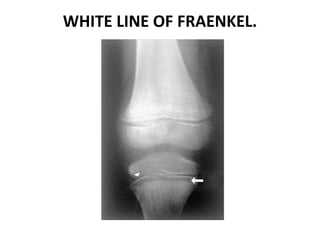
- Diagnosis is based on low vitamin C blood levels and x-ray findings of bone changes like the white line of Fraenkel. Treatment involves vitamin C supplementation in doses of at least 200mg daily until recovery is complete.