Downloaded 781 times





![The operative treatment of complex pilon fractures: A strategy
of soft tissue control
Xianfeng He, Yong Hu, [...], and Yon
gping Ruan IJO sep 2013
Two Stage treatment with
NPWT
36 Patients
one sup infection
no deep infection](https://image.slidesharecdn.com/pilonfractures-150928181249-lva1-app6891/85/Pilon-fractures-37-320.jpg)
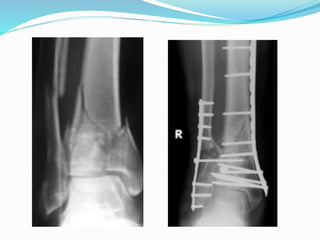





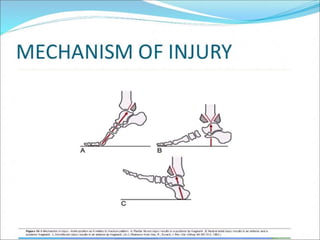
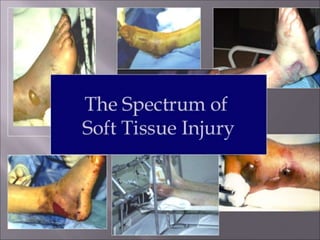
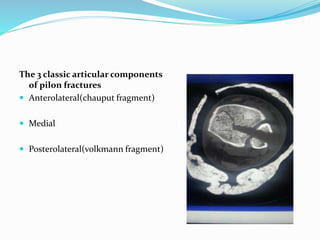
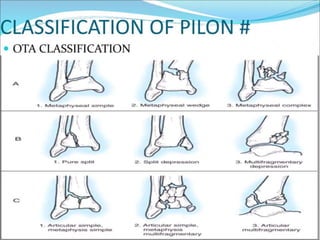
1) Pilon fractures involve injuries to the distal tibial articular surface and were first described in 1911. 2) They account for 5-7% of tibial fractures and result from high-energy impacts. 3) Treatment is challenging due to articular comminution, bone loss, and soft tissue injury. Surgical management aims to reconstruct the articular surface and metaphysis while treating soft tissues.























































































