Downloaded 422 times



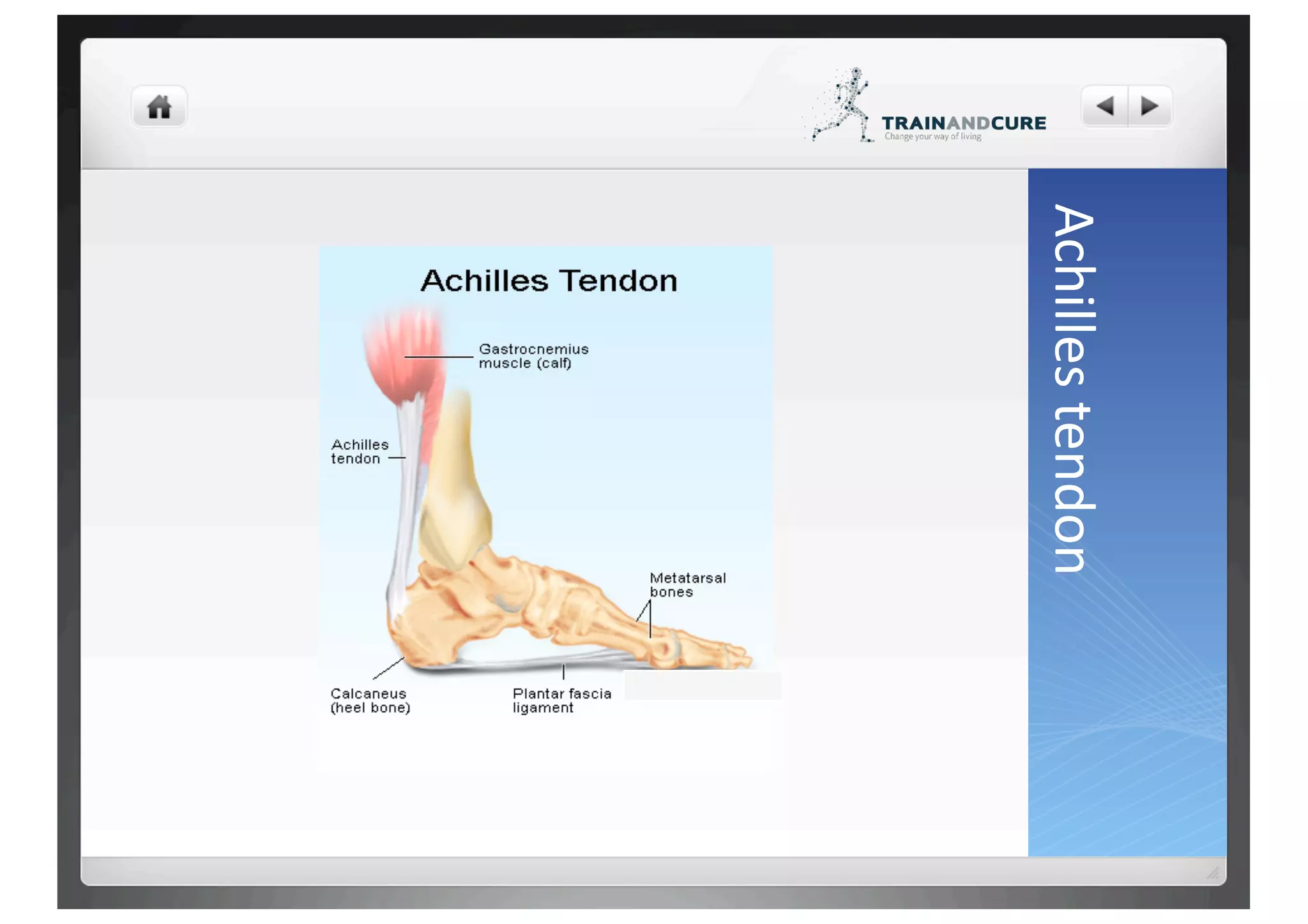





























The Achilles tendon connects the calf muscles to the heel bone and allows walking, running, and jumping by tightening as the calf muscles contract. Achilles tendon ruptures are most common in recreational athletes aged 30-50 and can result from a sudden forced movement of the foot or overuse. While nonsurgical treatment is a option, surgery is often recommended to repair the torn tendon and speed recovery through physical therapy.















































