Downloaded 311 times















![APC [B-Cell]
Th
Y
Ag
MHC-II P
B7 CD-28
TCR
CD-40 CD-40L
CK
CO-STIMULATORY SIGNALS
Nucleus
Singling
Cascades](https://image.slidesharecdn.com/tcim-150831071119-lva1-app6891/85/T-Cell-Mediated-Immunity-23-320.jpg)

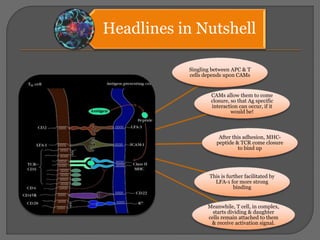
![As the T-Cells Adhere to
APC
Movements of TCR towards
the Peptide~MHC Starts
They come closure to each
other and bind
Thus the complex so formed
will be [T-CELLS-TCR-
PEPTIDE~MHC-APC]
• LFA-1 changes its confirmation
Binding become tighter
• This is required for the long time
to Activate the cells
After the receiving
stimulation signal T cells
starts dividing and its
progeny still attached to the
mother cells and received
activation signals
To activate the T cells APC
has to delivered two signals
• To TCR via MHC~Peptide
Complex
• Co-stimulatory signal via
interaction of B7 to CD-28](https://image.slidesharecdn.com/tcim-150831071119-lva1-app6891/85/T-Cell-Mediated-Immunity-26-320.jpg)




T cells are activated through the recognition of antigen peptides presented on MHC complexes on antigen presenting cells (APCs). This leads to T cell proliferation and differentiation into effector T cells. Cytotoxic T cells recognize endogenous antigens on MHC I to kill infected cells, while helper T cells recognize exogenous peptides on MHC II and secrete cytokines to stimulate macrophage activation or B cell antibody production. Full T cell activation requires both antigen recognition by the TCR and co-stimulatory signaling between molecules such as B7 and CD28.



















































![ANTIGEN PROCESSING PRESENTATION AND RECOGNITION - Copy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/antigenprocessingpresentationandrecognition-copyautosaved-220815200136-89a4c3c9-thumbnail.jpg?width=640&height=640&fit=bounds)























































