Downloaded 15 times
![Fig. 1. Wound healing is a
complex process
encompassing a number of
overlapping phases,
including inflammation,
epithelialization,
angiogenesis and matrix
deposition. During
inflammation, the
formation of a blood clot
re-establishes hemostasis
and provides a provisional
matrix for cell migration.
Cytokines play an
important role in the
evolution of granulation
tissue through recruitment
of inflammatory
leukocytes and stimulation
of fibroblasts and
epithelial cells. [Note:
figure is adapted from
reference 1.]](https://image.slidesharecdn.com/hemostsisthrombosis-150831064826-lva1-app6891/85/Hemostsis-thrombosis-9-320.jpg)
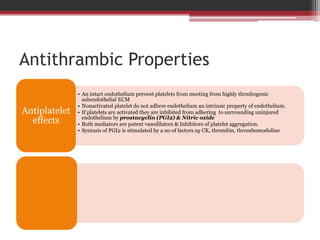
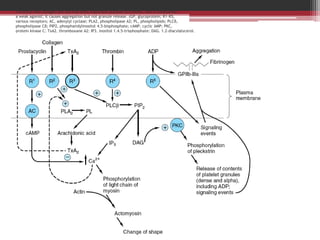

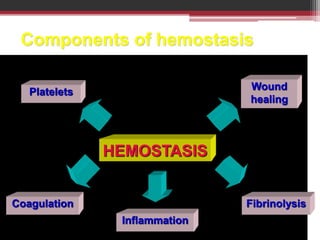
Hemostasis is the process by which blood is maintained in a fluid state within blood vessels, but forms clots to prevent blood loss when vessels are damaged. It involves three main components: primary hemostasis where platelets form a plug at the site of injury, secondary hemostasis where fibrin is formed to consolidate the platelet plug, and fibrinolysis which cleans up the clot once it is no longer needed. The process is tightly regulated to prevent inappropriate clot formation under normal conditions through properties of the endothelium like secretion of prostacyclin and nitric oxide. When vessels are damaged, factors like tissue factor activate the coagulation cascade leading to thrombin generation and fibrin clot formation to seal the break.






































































































