Downloaded 28 times



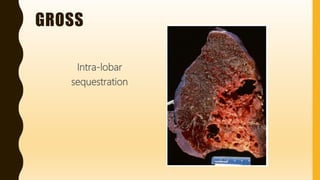
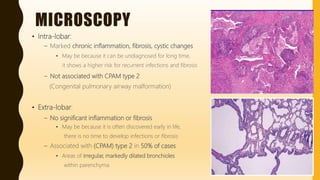



This document summarizes pulmonary sequestration, a congenital malformation where a nonfunctional lung lobe receives its blood supply from the systemic circulation rather than the pulmonary arteries. It can be either extra-lobar, located outside the lung, or intra-lobar, located within the lung. Intra-lobar sequestration is more common and often presents later in life, showing chronic inflammation and fibrosis from recurrent infections. Extra-lobar sequestration typically presents earlier and shows less inflammation since infections have less time to develop. Microscopically, intra-lobar sequestration displays marked chronic inflammation and fibrosis with cyst formation, while extra-lobar sequestration does not usually have























































































