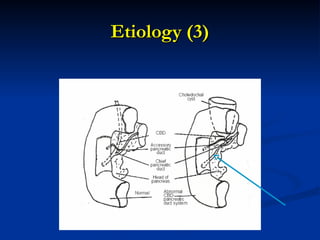
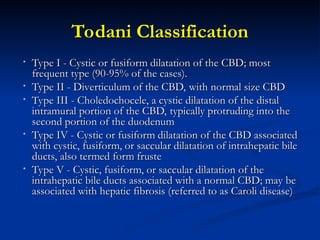
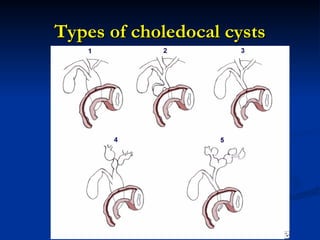
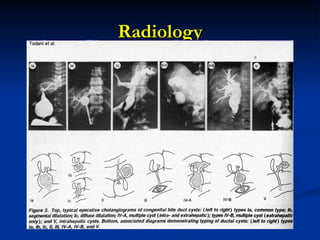
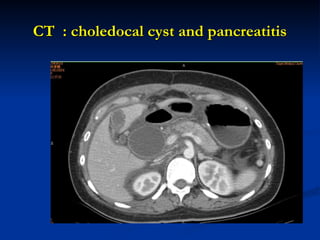
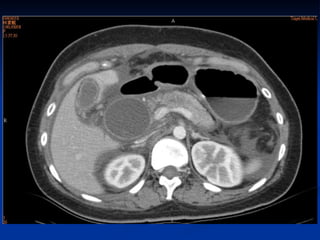
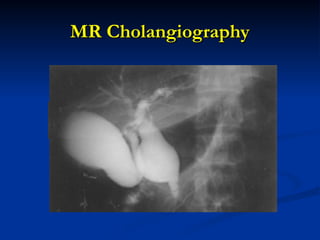
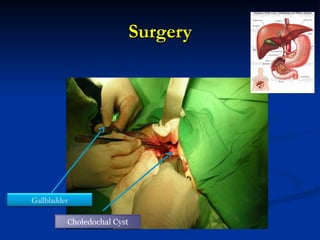
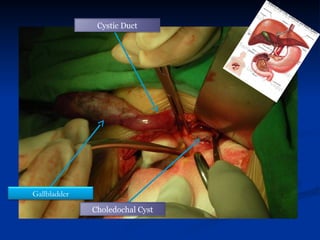
Choledochal cysts are congenital anomalies of the bile ducts, occurring in approximately 1 in 10,000 to 13,000 live births, and are more prevalent in women and Asians. They are classified into five types according to Todani's classification, with Type I being the most common. Complications include pancreatitis, cholangitis, and an increased risk of cholangiocarcinoma, with treatment options varying based on the type of cyst.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














