Topics
• Abdominal walldefects
• Omphalocele
• Gastroschisis
• Extrophy epispadius sprectrum
• Body stalk anomalies
• Disorder of biliary system liver and pancreas
• Billary atresia
• Choledocal cyst
• Cholelithiasis and acute cholecystitis
• Hepatic masses
• Pancreatic masses
• Burkitt lymphoma
3.
Abdominal wall defects
•omphalocele
• Definition: A birth defect where a baby's intestines or other organs
protrude through the abdomen at the belly button.
• Development: Normally, the fetal gut herniates into the umbilical cord
during development and then returns to the abdomen. In omphalocele, this
retraction is interrupted.
• Features:
• Umbilical cord insertion at the apex of the hernia.
• Three-layered membrane (peritoneum, Wharton's jelly, amnion)
covering the defect.
4.
Associated Conditions &Management
• Associated Conditions: High risk of other birth defects, especially heart and
gastrointestinal problems.
• Prenatal Diagnosis: Detected by ultrasound. Serial ultrasounds monitor size,
contents, and sac rupture.
5.
Abdominal wall defects:Gastroschisis
• Definition: A birth defect where the baby's intestines protrude through a
small hole in the abdominal wall, typically to the right of the umbillicus
• Key Features:
• Location: Right of the umbilical cord insertion.
• Membrane: No covering membrane.
• Size: Usually smaller than 2 cm.
• Associated Anomalies: Rare compared to omphalocele.
Management:
• Prenatal: Ultrasound diagnosis, fetal surveillance.
6.
Abdominal wall defects:Cloacal Exstrophy
• Definition: A rare and severe birth defect affecting the lower part of the
body.
• Pathogenesis: Results from an early breakdown of the cloacal membrane
during embryonic development.
• Manifestations: Involves the hindgut, bladder, genitalia, and often other
organ systems.
• Characteristic Feature: "Elephant trunk" appearance due to herniation of the
hindgut and bowel between the everted bladder halves.
Abdominal wall defects:Bladder Exstrophy
• Definition: A rare birth defect where the bladder wall is exposed
outside the body.
• Pathogenesis: Results from an incomplete closure of the lower
abdominal wall during embryonic development.
• Manifestations: Involves the urinary bladder and external genitalia.
• Key Features:
• Eversion of the posterior bladder wall.
• Absence of the anterior abdominal wall over the bladder.
9.
Abdominal wall defects:Bladder Exstrophy
Differential Diagnosis:
• Omphalocele: Differentiate by the absence of the bladder and the
superior position of the umbilical cord insertion.
• Management:
• Requires a multidisciplinary team approach.
• Complex surgical reconstruction in stages.
• Long-term follow-up for urinary incontinence and other complications.
• Management of associated conditions (e.g., epispadias, inguinal hernias).
10.
Epispadias, Prune BellySyndrome, and Other Abdominal Wall Defects
• Epispadias: Abnormal opening of the urethra along the dorsal surface of the
penis.
• Prune Belly Syndrome: Deficiency of abdominal wall musculature with
associated urinary tract abnormalities.
• Pentalogy of Cantrell: Midline supraumbilical abdominal defect, sternal
defect, diaphragmatic defects, cardiac abnormalities.
• Body Stalk Anomalies: Malformation of thorax, abdomen, or both, often
with craniofacial and limb defects.
11.
Congenital Diaphragmatic Hernia
•Definition: Herniation of abdominal contents into the chest cavity through a
defect in the diaphragm.
• Types: Bochdalek (posterior, more common, left-sided) and Morgagni
(anterior, right-sided).
• Complications: Lung hypoplasia, pulmonary hypertension.
• Management: Prenatal diagnosis (ultrasound), fetal therapy (tracheal
occlusion), postnatal surgical repair.
12.
Biliary Atresia: Pathophysiologyand Clinical Presentation
• Definition: A progressive cholestatic liver disease in infants characterized by the
absence or severe destruction of extrahepatic bile ducts.
• Pathophysiology: Likely an inflammatory process leading to bile duct fibrosis and
obliteration.
• Clinical Features:
• Progressive jaundice
• Dark urine
• Acholic stools
• Hepatomegaly
• Splenomegaly
• Pruritus (in later stages)
13.
Imaging and Managementof Biliary Atresia
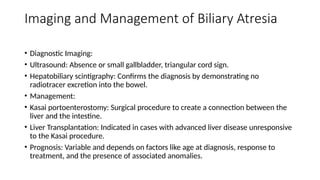
• Diagnostic Imaging:
• Ultrasound: Absence or small gallbladder, triangular cord sign.
• Hepatobiliary scintigraphy: Confirms the diagnosis by demonstrating no
radiotracer excretion into the bowel.
• Management:
• Kasai portoenterostomy: Surgical procedure to create a connection between the
liver and the intestine.
• Liver Transplantation: Indicated in cases with advanced liver disease unresponsive
to the Kasai procedure.
• Prognosis: Variable and depends on factors like age at diagnosis, response to
treatment, and the presence of associated anomalies.
14.
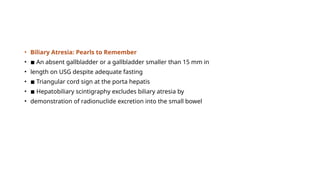
• Biliary Atresia:Pearls to Remember
• ◾ An absent gallbladder or a gallbladder smaller than 15 mm in
• length on USG despite adequate fasting
• ◾ Triangular cord sign at the porta hepatis
• ◾ Hepatobiliary scintigraphy excludes biliary atresia by
• demonstration of radionuclide excretion into the small bowel
15.
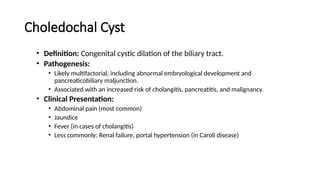
Choledochal Cyst
• Definition:Congenital cystic dilation of the biliary tract.
• Pathogenesis:
• Likely multifactorial, including abnormal embryological development and
pancreaticobiliary maljunction.
• Associated with an increased risk of cholangitis, pancreatitis, and malignancy.
• Clinical Presentation:
• Abdominal pain (most common)
• Jaundice
• Fever (in cases of cholangitis)
• Less commonly: Renal failure, portal hypertension (in Caroli disease)
16.
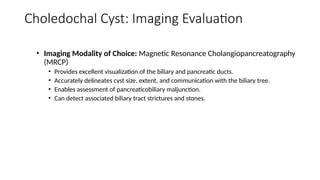
Choledochal Cyst: ImagingEvaluation
• Imaging Modality of Choice: Magnetic Resonance Cholangiopancreatography
(MRCP)
• Provides excellent visualization of the biliary and pancreatic ducts.
• Accurately delineates cyst size, extent, and communication with the biliary tree.
• Enables assessment of pancreaticobiliary maljunction.
• Can detect associated biliary tract strictures and stones.
17.
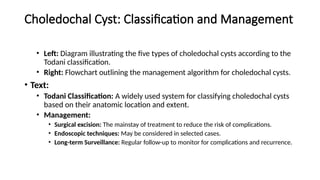
Choledochal Cyst: Classificationand Management
• Left: Diagram illustrating the five types of choledochal cysts according to the
Todani classification.
• Right: Flowchart outlining the management algorithm for choledochal cysts.
• Text:
• Todani Classification: A widely used system for classifying choledochal cysts
based on their anatomic location and extent.
• Management:
• Surgical excision: The mainstay of treatment to reduce the risk of complications.
• Endoscopic techniques: May be considered in selected cases.
• Long-term Surveillance: Regular follow-up to monitor for complications and recurrence.
18.
• Choledochal Cyst:Pearls to Remember
• ◾ The Todani classification divides choledochal cyst into five main
• subtypes.
• ◾ Type 5 cyst or Caroli disease complicated by hepatic fibrosis is
• known as called Caroli syndrome.
• ◾ The central dot sign refers to an ectatic intrahepatic biliary duct
• surrounding an enhancing portal vein in Caroli disease.
19.
Cholelithiasis in thePediatric Population: Risk
Factors and Imaging
• Definition: Cholelithiasis refers to the presence of gallstones within the
gallbladder.
• Risk Factors:
• Hemolytic anemias (e.g., sickle cell disease, thalassemia)
• Cystic fibrosis
• Obesity
• Prolonged parenteral nutrition
• Certain genetic disorders
• Imaging Modalities:
• Ultrasound: The initial imaging modality of choice, demonstrating the presence, number,
and size of gallstones.
• Magnetic Resonance Cholangiopancreatography (MRCP): May be utilized in cases of
equivocal ultrasound findings or to further evaluate biliary tract anatomy.
20.
Acute Cholecystitis inPediatrics: Clinical Presentation and
Management
• Definition: Acute cholecystitis is an inflammatory condition of the gallbladder, typically
caused by gallstone obstruction of the cystic duct.
• Clinical Presentation:
• Right upper quadrant abdominal pain (often colicky)
• Fever
• Nausea and vomiting
• Leukocytosis
• Management:
• Medical Management: Antibiotic therapy, pain control, hydration.
• Surgical Management:
• Laparoscopic cholecystectomy is the gold standard treatment for symptomatic cholelithiasis and acute
cholecystitis.
• Indications for early surgical intervention include severe symptoms, biliary sepsis, and high-risk comorbidities.
21.
Hepatic Hemangiomas inChildren: An Overview
• Introduction: Hepatic hemangiomas are the most common benign liver
tumors in children.
• Classification:
• Congenital: Present at birth, may exhibit rapid involution or remain static.
• Infantile: Develop after birth, typically undergo a period of rapid growth followed by
involution.
• Clinical Significance: Range from asymptomatic to life-threatening, with
potential for complications such as high-output cardiac failure and
thrombocytopenia.
22.
Imaging Evaluation ofHepatic Hemangiomas
Ultrasound:
• Variable echogenicity (hypoechoic to hyperechoic).
• Prominent vascularity on Doppler ultrasound.
• May demonstrate internal cystic areas or flow voids.
• MRI:
• T1 hypointense, T2 hyperintense on conventional sequences.
• Characteristic progressive centripetal enhancement on dynamic contrast-enhanced MRI.
• May demonstrate flow voids within the lesion.
23.
Management of HepaticHemangiomas in Children
• Image:
• Left: Flowchart outlining the management algorithm for hepatic hemangiomas.
• Right: Diagram illustrating potential complications of large or symptomatic
hemangiomas (e.g., high-output cardiac failure).
• Text:
• Management:
• Observation: For asymptomatic, small lesions.
• Medical Therapy: Propranolol (first-line), corticosteroids for symptomatic lesions.
• Interventional Procedures: Embolization, radiofrequency ablation in selected cases.
• Surgical Resection: Reserved for complex cases or those with life-threatening complications.
• Prognosis: Most infantile hemangiomas undergo spontaneous involution. Prognosis
for congenital hemangiomas varies depending on size and associated complications.
24.
Mesenchymal Hamartoma ofthe Liver
• Definition: The second most common benign liver tumor in children.
• Clinical Presentation: Typically presents in young children with painless
abdominal distension.
• Imaging:
• Ultrasound: Multilocular cystic mass with low-level internal echoes.
• MRI: Characteristic T1 hypointense and T2 hyperintense signal.
• Management: Surgical resection is the treatment of choice due to the
potential for growth and rare malignant transformation.
Hepatoblastoma: Imaging Featuresand Staging
• Imaging:
• CT: Heterogeneous enhancement, calcifications, possible vascular invasion.
• MRI: Detailed assessment of tumor extent and vascular involvement.
• PRETEXT Staging: A crucial prognostic factor for treatment planning.
• Based on the number of contiguous liver segments free of tumor involvement.
• Guides treatment decisions (surgery, chemotherapy, liver transplantation).
27.
Hepatoblastoma: Management andPrognosis
• Treatment:
• Surgery: Primary treatment modality.
• Neoadjuvant Chemotherapy: Used to reduce tumor burden prior to surgery.
• Liver Transplantation: Considered for unresectable or recurrent disease.
• Prognosis: Overall prognosis is favorable with advancements in treatment.
Prognostic factors include tumor stage, age at diagnosis, and response to
chemotherapy
28.
• Hepatoblastoma: Pearlsto Remember
• ◾ Most common pediatric hepatic malignancy occurring before the
• age of 5 years
• ◾ Well-defined tumors with lobulated contours and heterogeneous
• enhancement
• ◾ Calcifications are present in more than half of these tumors.
• ◾ The PRETEXT classification is used for risk stratification.
29.
Hepatocellular Carcinoma (HCC)in Children
• Definition: Primary liver cancer arising from hepatocytes.
• Risk Factors: Biliary atresia, glycogen storage disease, α1-antitrypsin
deficiency, Wilson disease.
• Clinical Presentation: Abdominal distension, weight loss, anorexia, elevated
serum alpha-fetoprotein (AFP) levels.
• Imaging:
• CT: Hypervascular mass with variable enhancement patterns.
• MRI: Characterization of tumor extent and vascular invasion.
30.
Fibrolamellar Hepatocellular Carcinoma
•Definition: A rare variant of HCC with a distinct clinical and pathological
profile.
• Key Features:
• Occurs in adolescents and young adults.
• Typically lacks a background liver disease.
• Characterized by a central fibrous scar (hypointense on T2-weighted MRI, often
calcified).
• Normal or only mildly elevated AFP levels.
31.
Undifferentiated Embryonal Sarcomaof the Liver
• Definition: A rare, aggressive hepatic malignancy with a predominantly
mesenchymal origin.
• Clinical Presentation: Abdominal distension, weight loss, anorexia.
• Imaging:
• Typically appears as a large, cystic mass on imaging.
• May demonstrate internal septations, hemorrhage, and areas of solid enhancement.
• Prognosis: Aggressive tumor with a high risk of recurrence and metastasis.
32.
Management of HepaticMalignancies in Children
• Treatment Strategies:
• Surgery: Primary treatment option for resectable tumors.
• Chemotherapy: Neoadjuvant and adjuvant chemotherapy for hepatoblastoma.
• Liver Transplantation: Considered for unresectable or recurrent disease.
• Prognosis: Varies depending on the specific tumor type, stage, and response
to treatment.
• Importance of Multidisciplinary Care: Collaboration between oncologists,
surgeons, radiologists, and pathologists is crucial for optimal patient
outcomes.
33.
Pancreatic Pseudocysts andCystic Neoplasms
• Pseudocysts: Most common type of pancreatic cyst in children, typically
resulting from pancreatitis or trauma.
• Cystic Neoplasms:
• Solid and Papillary Epithelial Neoplasm (SPEN): Most common pancreatic neoplasm in
children, predominantly affecting females.
• Congenital Cystic Neoplasms: Rare, may be associated with genetic syndromes.
34.
Pancreatoblastoma and OtherPancreatic Tumors
• Pancreatoblastoma: Rare but aggressive malignant tumor; may be associated
with Beckwith-Wiedemann syndrome.
• Other Tumors:
• Endocrine tumors (insulinomas, gastrinomas).
• Neuroendocrine tumors.
• Lymphoma (e.g., Burkitt lymphoma).
• Metastatic disease.
35.
Burkitt Lymphoma: AHigh-Grade Lymphoma
with Pancreatic Involvement
• Definition: An aggressive B-cell non-Hodgkin lymphoma.
• Clinical Presentation: Abdominal pain, constipation, fever, weight loss.
• Imaging:
• CT: Demonstrates extranodal masses, bowel wall thickening, and potential for solid organ
involvement (liver).
• PET/CT: Valuable for assessing disease extent and response to treatment.
• Management: Chemotherapy is the mainstay of treatment.
Editor's Notes
#3 Normally during development, the fetal bowel loops herniate through the
developing anterior abdominal wall into the umbilical cord during the 6th to
10th weeks of gestation (see Fig. 84.1). Interrupted bowel retraction into the
abdominal cavity results in omphalocele [47]. Understanding this process
explains the characteristic umbilical cord insertion at the apex of the hernia
sac and the three-layered membrane composed of peritoneum, Wharton jelly,
and amnion covering the defect (Fig. 84.48) [48]. Associated congenital
anomalies are frequently noted in cases of omphalocele, the most common of
which are cardiac and GI in nature. The condition is associated with a high
risk of underlying genetic abnormalities. In utero detected omphalocele
require serial ultrasound monitoring to evaluate the size of the omphalocele
and its contents, exclude in utero sac rupture, and determine the route of
delivery [
#5 Gastroschisis is a paraumbilical ventral body wall defect with secondary
midgut herniation into the amniotic cavity. This defect is most commonly to
the right of cord insertion, not covered by amniotic membrane, and
characteristically smaller than 2 cm (Fig. 84.49). Compared with
omphalocele, gastroschisis is rarely associated with congenital
abnormalities [50]. Also, underlying genetic abnormalities are uncommon in
cases of isolated gastroschisis. Postnatal outcome is mainly dependent on the
bowel condition at birth with 95% survival rate in cases of uncomplicated
gastroschisis.
#6 Cloacal Exstrophy
Cloacal exstrophy occurs secondary to early breakdown of the cloacal
membrane, resulting in a severe abnormality involving the lower half of the
body, namely the hindgut, bladder, and genitalia. The associated
characteristic elephant trunk appearance represents herniation of the
hindgut and bowel between the everted two bladder halves [51]. Cloacal
exstrophy is frequently associated with other renal anomalies, including
renal agenesis, cystic dysplasia, and ectopia. Associated extrarenal
abnormalities include lower extremity defects, ascites, a narrow thorax, and
a single umbilical artery. Cloacal exstrophy can also be a part of the
Omphalocele, Exstrophy Bladder, Imperforate anus, and Spinal anomalies
(OEIS) complex, in which cloacal exstrophy is associated with omphalocele,
imperforate anus, and spinal defects. The neonatal prognosis depends on the
severity of the defect and associated malformations [
#8 Bladder exstrophy occurs from incorrect retraction of the cloacal membrane,
leading to eversion of the bladder plate. The resultant abnormality involves
only the urinary bladder and external genitalia (Fig. 84.50). The normal
hindgut differentiates this anomaly from cloacal exstrophy. To differentiate
bladder exstrophy from omphalocele, it is important to document the
absence of the bladder and the position of the umbilical cord insertion
superior to the ventral abdominal wall defect [51].
#12 Biliary Atresia
Biliary atresia is thought to arise secondary to an in-utero progressive
postinflammatory process with subsequent absent or severely deficient
extrahepatic biliary tree. It usually presents in the neonatal period with
progressive obstructive jaundice. Death is expected by 2 years of age in
untreated cases because of the development of secondary biliary cirrhosis
[39]. In 20% of cases, biliary atresia is associated with situs anomalies and
is called biliary atresia-splenic malformation syndrome.
The gold standard to diagnose biliary atresia is biopsy and intraoperative
cholangiogram. Imaging helps establish the diagnosis, especially
differentiating it from neonatal hepatitis, and allows establishing to an
appropriate plan of management [60]. Imaging is the initial imaging
modality of choice in cases of neonatal jaundice.
◾ An absent gallbladder or a gallbladder smaller than 15 mm in length on ultrasound despite
adequate fasting is 84.8% sensitive and 76.9% specific for biliary atresia.
◾ On the other hand, a triangular focus of echogenic tissue at the porta hepatis, also known as
the triangular cord sign, is reported to be 96% accurate, 23.3% to 100% sensitive, and 89%
to 100% specific for diagnosing biliary atresia [61].
◾ Hepatobiliary scintigraphy can exclude biliary atresia by demonstration of radionuclide
excretion into the small bowel (Fig. 84.52) [62,63]. Cases of neonatal hepatitis demonstrate
poor hepatic radiotracer uptake and delayed radiotracer excretion into the bowel.
FIGURE 84.52 Transverse grayscale ultrasound from a 5-week-old
boy with conjugated hyperbilirubinemia shows absent gallbladder
despite adequate fasting in biliary atresia (A). Planar anterior and
posterior hepatobiliary iminodiacetic acid scan acquired 24 hours after
injection of the radiotracer shows adequate radiotracer uptake in the
liver without contrast excretion into the duodenum (B).
Patients with biliary atresia are commonly treated surgically through
creating a hepatic portoenterostomy, also known as the Kasai procedure.
Cases that develop biliary cirrhosis and end-stage liver disease usually
require liver transplantation [64].
#15
Left: Diagram illustrating the normal biliary tree and a choledochal cyst.
Right: Histological image demonstrating dilated bile ducts (if available).
#16 Left: Ultrasound image showing a type I choledochal cyst.
Right: MRCP image demonstrating a type III choledochal cyst (choledochocele).
#17 Left: Diagram illustrating the five types of choledochal cysts according to the Todani classification.
Right: Flowchart outlining the management algorithm for choledochal cysts.
#19 Left: Ultrasound image demonstrating multiple gallstones within the gallbladder (similar to Fig. 84.58).
Right: Diagram illustrating risk factors for gallstone formation in children.
Cholelithiasis and Acute Cholecystitis
Major risk factors for gallstones in the pediatric population include
hemolytic anemias, cystic fibrosis, obesity, and parenteral nutrition [71].
Similar to the adult population, USG is the mainstay for biliary stones
evaluation (Figs. 84.58 and 84.59). MRCP can be used in equivocal cases
and shows calculi as areas of signal void within the biliary tree. In contrast
to the adult population, 30% of pediatric cases are acalculous in nature.
Cholecystectomy is the treatment of choice for symptomatic gallstone
disease and in patients with high-risk comorbidities such as hemolytic
anemias [72].
FIGURE 84.58 Longitudinal grayscale ultrasound from a 16-year-old
young woman with sickle-cell anemia shows multiple calculi within a
distended gallbladder (GB).
FIGURE 84.59 Transverse grayscale ultrasound image from a 12-
year-old girl with shock of unclear origin demonstrates a grossly
thickened gallbladder wall (GB) and pericholecystic fluid in keeping with
acalculous cholecystitis
#20 Image:
Ultrasound image demonstrating gallbladder wall thickening and pericholecystic fluid (similar to Fig. 84.59).
#21 Left: Histological image of a hepatic hemangioma (if available).
Right: Diagram illustrating the spectrum of hepatic masses in children.
#22 Left: Ultrasound image demonstrating a large, heterogeneous hepatic hemangioma with prominent vascularity.
Right: MRI images showing a hepatic hemangioma with characteristic signal intensity and progressive centripetal enhancement.
#23 Image:
Left: Flowchart outlining the management algorithm for hepatic hemangiomas.
Right: Diagram illustrating potential complications of large or symptomatic hemangiomas (e.g., high-output cardiac failure).
#24 Image:
Left: Ultrasound image demonstrating a multilocular, cystic mesenchymal hamartoma.
Right: Diagram illustrating the spectrum of hepatic masses in children.
#25 Left: Photomicrograph of a hepatoblastoma (if available).
Right: Diagram illustrating the spectrum of hepatic malignancies in children.
#26 Left: CT scan demonstrating a large, heterogeneous hepatoblastoma with areas of calcification.
Right: Diagram illustrating the PRETEXT staging system for hepatoblastoma.
#27 Left: Diagram illustrating the treatment algorithm for hepatoblastoma.
Right: Illustration of potential metastatic sites (e.g., lungs).
#29 Left: Diagram illustrating risk factors for HCC in children (e.g., biliary atresia, glycogen storage disease).
Right: CT scan demonstrating a solitary, hypervascular hepatic mass suggestive of HCC.
#30 Left: MRI images demonstrating a fibrolamellar HCC with a central hypointense scar.
Right: CT scan showing a fibrolamellar HCC with calcifications within the central scar.
#31 Left: Ultrasound image demonstrating a cystic-appearing embryonal sarcoma.
Right: MRI images showing a heterogeneous, lobulated embryonal sarcoma with areas of hemorrhage.
#32 Left: Flowchart illustrating the treatment algorithm for hepatoblastoma.
Right: Diagram illustrating potential sites of metastasis for hepatic malignancies (e.g., lungs, bone).
#33 Left: Ultrasound image demonstrating a large pancreatic pseudocyst.
Right: CT scan showing a well-defined, cystic pancreatic mass (likely a cystic neoplasm).
#34 Left: CT scan demonstrating a pancreatoblastoma with heterogeneous enhancement and possible calcifications.
Right: Diagram illustrating the spectrum of pancreatic tumors in children.
#35 Left: CT scan demonstrating diffuse gastric wall thickening due to Burkitt lymphoma.
Right: PET/CT scan showing intense FDG uptake in multiple abdominal lymph nodes, suggestive of Burkitt lymphoma.







































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)









