Downloaded 22 times

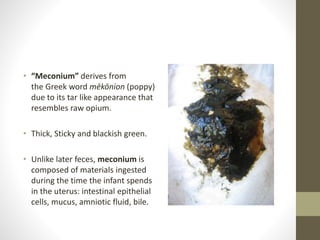

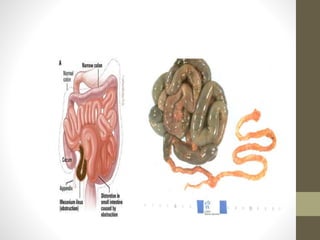
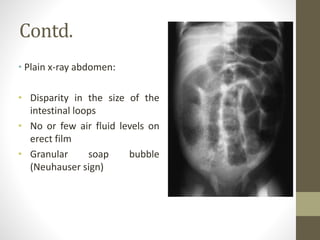
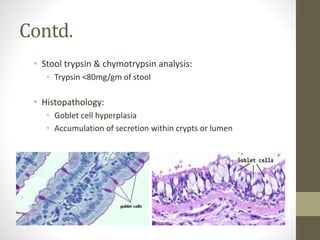

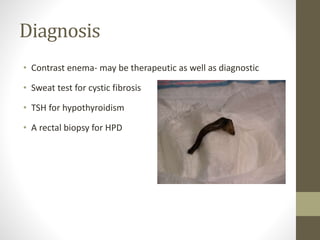



This document discusses meconium disease, specifically meconium ileus and meconium plug syndrome. Meconium ileus is a common cause of neonatal intestinal obstruction characterized by thick, viscid meconium in the ileum causing obstruction. It is often associated with cystic fibrosis. Treatment may involve contrast enemas or surgery like enterotomy. Meconium plug syndrome is the failure to pass a firm meconium plug, which can cause obstruction. It is usually treated with contrast enemas. Early diagnosis and treatment of meconium diseases is important for the well-being of newborns.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



